Anatomy
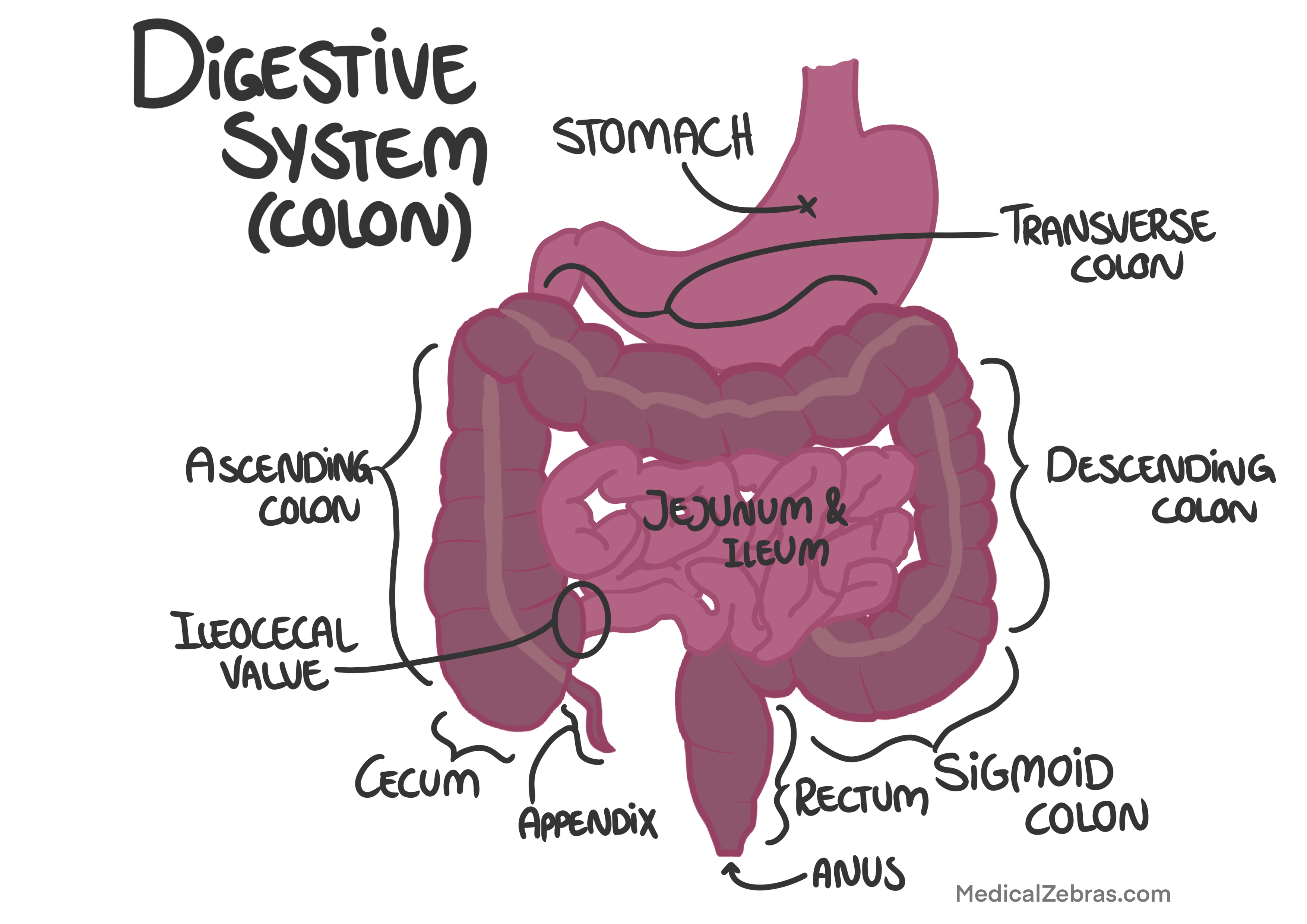
The cecum, colon and rectum is a long, tube-like organ, about 1.5 meters (5 feet) in length in an average adult, that together make up the large intestine in the digestive system. It is responsible for absorbing water and electrolytes from indigestible food matter and forming solid waste (feces) for elimination. The colon is further divided into several sections:- Cecum: This is the beginning of the large intestine, where the small intestine empties its contents.
- Ascending colon: This section starts at the cecum (where the small intestine meets the large intestine) and extends upward on the right side of the abdomen.
- Transverse colon: This section runs horizontally across the abdomen from the right to the left side.
- Descending colon: This section descends down the left side of the abdomen.
- Sigmoid colon: This S-shaped section connects the descending colon to the rectum.
- Rectum: The final section of the colon that stores feces before they are eliminated through the anus.
Function
The primary functions of the colon include:- Water absorption: The colon absorbs water and electrolytes from the remaining indigestible food matter, helping to maintain the body's fluid balance.
- Formation of feces: As water is absorbed, the remaining material solidifies into feces, which are then stored in the rectum until they are ready to be eliminated.
- Bacterial fermentation: The colon houses a large population of beneficial bacteria that help break down certain undigested carbohydrates through fermentation, producing gases and short-chain fatty acids that can be absorbed and used by the body.
- Immune function: The colon plays a role in immune function by housing gut-associated lymphoid tissue (GALT) that helps protect against pathogens.
Arterial supply
The colon receives its blood supply from branches of the superior and inferior mesenteric arteries:-
Superior mesenteric artery: This artery
supplies blood to the cecum, ascending colon, and the proximal
two-thirds of the transverse colon through branches such as the
ileocolic, right colic, and middle colic arteries.
- Ileocolic artery: Supplies the cecum and the beginning of the ascending colon.
- Right colic artery: Supplies the ascending colon.
- Middle colic artery: Supplies the proximal two-thirds of the transverse colon.
-
Inferior mesenteric artery: This artery
supplies blood to the distal one-third of the transverse colon,
descending colon, sigmoid colon, and rectum through branches
such as the left colic, sigmoid, and superior rectal arteries.
- Left colic artery: Supplies the distal one-third of the transverse colon and the descending colon.
- Sigmoid arteries: Supply the sigmoid colon.
- Superior rectal artery: Supplies the rectum.

Venous drainage
The venous drainage of the colon parallels its arterial supply and is primarily through the superior and inferior mesenteric veins:- Superior mesenteric vein: This vein drains blood from the cecum, ascending colon, and transverse colon. It eventually joins with the splenic vein to form the portal vein, which carries blood to the liver for detoxification and nutrient processing.
- Inferior mesenteric vein: This vein drains blood from the descending colon, sigmoid colon, and rectum. It typically drains into the splenic vein, which then joins the superior mesenteric vein to form the portal vein.
Lymphatic drainage
The lymphatic drainage of the colon follows its arterial supply and is essential for immune function and the removal of waste products:- Lymph from the cecum and ascending colon drains into the ileocolic and right colic lymph nodes, which then drain into the superior mesenteric lymph nodes.
- Lymph from the transverse colon drains into the middle colic lymph nodes, which also drain into the superior mesenteric lymph nodes.
- Lymph from the descending colon drains into the left colic lymph nodes, which then drain into the inferior mesenteric lymph nodes.
- Lymph from the sigmoid colon drains into the sigmoid lymph nodes, which also drain into the inferior mesenteric lymph nodes.
- Lymph from the rectum drains into the pararectal lymph nodes, which then drain into the inferior mesenteric lymph nodes and internal iliac lymph nodes.
Nerve supply
The nerve supply to the colon is provided by both the autonomic and enteric nervous systems:- Autonomic nervous system: The sympathetic nerve supply to the colon arises from the thoracolumbar region of the spinal cord (T10-L2) and is conveyed via the superior and inferior mesenteric plexuses. Sympathetic stimulation generally inhibits peristalsis and promotes vasoconstriction. The parasympathetic nerve supply arises from the vagus nerve (cranial nerve X) for the proximal two-thirds of the colon and from the pelvic splanchnic nerves (S2-S4) for the distal one-third of the colon. Parasympathetic stimulation promotes peristalsis and increases secretions.
- Enteric nervous system: The enteric nervous system, often referred to as the "second brain" of the gut, is a complex network of neurons located within the walls of the gastrointestinal tract. It regulates various functions of the colon, including motility, secretion, and blood flow, largely independent of the central nervous system.
Histology
The histology of the colon is characterized by several distinct features that reflect its specialized functions in absorption and feces formation:- Mucosa: The innermost layer of the colon is the mucosa, which is lined by simple columnar epithelium. This layer contains numerous goblet cells that secrete mucus to lubricate the passage of feces. The mucosa also has crypts of Lieberkühn, which are glandular structures that produce intestinal juices.
- Submucosa: Beneath the mucosa lies the submucosa, a layer of connective tissue that contains blood vessels, lymphatics, and nerves. This layer provides support to the mucosa and facilitates nutrient absorption.
- Muscularis externa: The muscularis externa consists of two layers of smooth muscle: an inner circular layer and an outer longitudinal layer. The outer longitudinal layer is organized into three distinct bands called taeniae coli, which help in the contraction and movement of the colon.
- Serosa: The outermost layer of the colon is the serosa, a thin layer of connective tissue covered by a layer of mesothelium. The serosa provides protection and reduces friction between the colon and surrounding organs.
Immune function: The colon contains gut-associated lymphoid tissue (GALT) within its mucosa and submucosa, which plays a crucial role in immune surveillance and response to pathogens.
Pathology
Diverticulosis
Diverticulosis is a condition characterized by the formation of small, bulging pouches (diverticula) in the lining of the colon. These pouches develop when weak spots in the colon wall give way under pressure from the inside of the colon. Diverticulosis is common, especially in older adults, and often does not cause any symptoms. However, when the diverticula become inflamed or infected, the condition is called diverticulitis. Risk factors for diverticulosis include a low-fiber diet, obesity, and lack of physical activity. Treatment typically involves dietary changes, such as increasing fiber intake, and in severe cases, antibiotics or surgery may be required.Diverticulitis
Diverticulitis is an inflammation or infection of the diverticula in the colon. It occurs when one or more diverticula become blocked with waste material, leading to inflammation and sometimes infection.
Causes:
- Blocked diverticula
- Poor diet low in fiber
- Obesity
- Lack of physical activity
Symptoms:
- Abdominal pain
- Fever
- Changes in bowel habits
Diagnosis:
- Physical examination: Abdominal tenderness, especially in the lower left quadrant where the diverticula are commonly located (in the sigmoid colon).
- CT scan: Abdominal CT scan to visualize the colon and detect inflammation or complications. Shows thickening of the colon wall, presence of diverticula, and possible abscess formation.
- Blood tests: Complete blood count (CBC), C-reactive protein (CRP)
Treatment:
- Antibiotics: have to cover common gut bacteria such as E. coli and Bacteroides species. Often a combination of metronidazole and a fluoroquinolone or a beta-lactam/beta-lactamase inhibitor.
- Dietary changes: increasing fiber intake to improve bowel regularity and reduce pressure on the colon walls.
- Surgery in severe cases: may involve removal of the affected portion of the colon.
Ulcerative Colitis
Ulcerative colitis is a chronic inflammatory bowel disease (IBD) that affects the large intestines (sometimes also seen in the few last cm of the distal ileum, called backwash ileitis, as a result of severe colonic inflammation that "splashes back" into the ileum). It is characterized by inflammation and ulceration of the mucosal lining, the innermost lining of the colon, leading to symptoms such as abdominal pain, diarrhea (often bloody), and rectal bleeding.Smoking is actually associated with a lower risk of ulcerative colitis (and milder disease course), in contrast to Crohn's disease where smoking is a risk factor.
Peak age of onset is between 15-30 years, with a smaller second peak between 50-70 years.
The disease typically starts in the rectum and may extend proximally in a continuous manner to involve other parts of the colon. The severity of the disease can vary from mild to severe, and it may have periods of remission and flare-ups. Complications of ulcerative colitis can include an increased risk of colon cancer (which correlates with disease duration and severity, which is why regular surveillance colonoscopies are recommended), severe bleeding, and perforation of the colon.
Causes: the exact cause of ulcerative colitis is
unknown, but it is believed to result from a combination of factors:
- Genetic predisposition
- Immune system dysfunction
- Environmental factors, such as diet and stress
Symptoms:
- Abdominal pain and cramping, often in the lower left quadrant as the sigmoid colon is commonly affected
- Diarrhea, often with blood or pus
- Rectal bleeding, sometimes accompanied by mucus
- Urgency to defecate, often with a feeling of incomplete evacuation
- Weight loss, as a result of malabsorption and decreased appetite
- Fatigue, due to chronic inflammation and anemia
Diagnosis:
- Clinical evaluation: assessment of symptoms and medical history
-
Colonoscopy with biopsy: the gold standard for diagnosis.
- Continuous inflammation starting from the rectum
- Ulcerations and pseudopolyps (raised areas of inflamed tissue)
- Mucosal erythema (redness) and edema (swelling)
- Loss of vascular pattern
- Mucosal inflammation with crypt abscesses
- Goblet cell depletion
- Chronic inflammatory infiltrate in the lamina propria
Macroscopic findingsMicroscopic findings
Treatment:
- Anti-inflammatory medications, such as aminosalicylates and corticosteroids
- Immunosuppressants, such as azathioprine and cyclosporine
- Biologic therapies, such as infliximab and adalimumab
- Surgery in severe cases where the affected portion of the colon may need to be removed. Often done if medical therapy fails or complications arise, such as perforation, severe bleeding, , or toxic megacolon.
Crohn's Disease
Crohn's disease is a chronic inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal tract, from the mouth to the anus. However, it most commonly affects the end of the small intestine (ileum) and the beginning of the large intestine (colon). Crohn's disease is characterized by inflammation that can penetrate through multiple layers of the intestinal wall (called transmural inflammation if it affects all layers), leading to a variety of symptoms such as abdominal pain, diarrhea, weight loss, and fatigue. The inflammation can also cause complications such as strictures (narrowing of the intestines), fistulas (abnormal connections between different parts of the intestine or between the intestine and other organs), and abscesses.Unlike ulcerative colitis, which affects only the colon and rectum in a continuous manner, Crohn's disease can affect any part of the digestive tract in a patchy distribution, with healthy areas of tissue in between inflamed areas.
Causes: the exact cause of Crohn's disease is
unknown, but it is believed to result from a combination of factors:
- Genetic predisposition
- Immune system dysfunction
- Environmental factors, such as smoking and diet
Symptoms:
- Abdominal pain and cramping
- Diarrhea, which may be bloody
- Weight loss, as a result of malabsorption and decreased appetite
- Fatigue, due to chronic inflammation and nutrient deficiencies
- Fever, often low-grade because of ongoing inflammation
- Mouth sores, also known as aphthous ulcers
Diagnosis:
- Clinical evaluation: assessment of symptoms and medical history
-
Endoscopy with biopsy: colonoscopy or upper endoscopy to visualize
the affected areas and obtain tissue samples.
- Skip lesions (patchy areas of inflammation)
- Cobblestone appearance of the mucosa
- Fissures and fistulas
- Transmural inflammation (involving all layers of the bowel wall; mucosal, submucosal, muscularis propria, and serosa, which is in contrast to ulcerative colitis which only involves the mucosa)
- Inflammatory cell infiltration; lymphocytes, plasma cells, macrophages, and neutrophils
- Crypt architectural distortion; irregularly shaped and branched crypts
- Granulomas (clusters of immune cells)
- Fissuring ulcers; deep linear ulcers that can penetrate the bowel wall
- Fibrosis; thickening and scarring of connective tissue, which is a response to chronic inflammation and often a cause of strictures as it narrows the bowel lumen
- Crypt abscesses; collections of neutrophils within the crypts
Macroscopic findingsMicroscopic findings
Treatment:
- Anti-inflammatory medications, such as aminosalicylates and corticosteroids
- Immunosuppressants, such as azathioprine and methotrexate
- Biologic therapies, such as infliximab and adalimumab
- Surgery in severe cases where damaged portions of the intestine may need to be removed. Often done if medical therapy fails or complications arise, such as strictures, fistulas, or abscesses.
Collagenous Colitis
Collagenous colitis is a type of microscopic colitis, a chronic inflammatory condition of the colon that primarily affects older adults, particularly women. It is characterized by chronic, watery non-bloody diarrhea and abdominal pain. The exact cause of collagenous colitis is unknown, but it is believed to involve an abnormal immune response in the colon.
Symptoms:
- Chronic watery diarrhea
- Abdominal pain and cramping
- Weight loss
- Fatigue
Diagnosis:
-
Colonoscopy with biopsy: the gold standard for diagnosis.
- Thickened subepithelial collagen band (>10 micrometers)
- Increased inflammatory cells in the lamina propria including lymphocytes and plasma cells. The inflammation is typically mild to moderate, without significant crypt distortion.
- Epithelial damage, such as surface epithelial flattening and detachment
Macroscopic findings: usually normal appearance of the colon mucosa appearance of the colon mucosaMicroscopic findings:
Treatment:
- Anti-diarrheal medications, such as loperamide, to manage symptoms
- Anti-inflammatory medications, such as budesonide, to reduce inflammation
- Immunosuppressants, such as azathioprine, in severe cases
- Dietary changes, such as avoiding caffeine and lactose, to help manage symptoms
Lymphocytic Colitis
Lymphocytic colitis is a type of microscopic colitis, a chronic inflammatory condition of the colon that primarily affects older adults, particularly women. It is characterized by chronic, watery non-bloody diarrhea and abdominal pain. The exact cause of lymphocytic colitis is unknown, but it is believed to involve an abnormal immune response in the colon.
Symptoms:
- Chronic watery diarrhea
- Abdominal pain and cramping
- Weight loss
- Fatigue
Diagnosis:
-
Colonoscopy with biopsy: the gold standard for diagnosis.
- Increased intraepithelial lymphocytes (>20 lymphocytes per 100 epithelial cells)
- Increased inflammatory cells in the lamina propria, including lymphocytes and plasma cells. The inflammation is typically mild to moderate, without significant crypt distortion.
- Epithelial damage, such as surface epithelial flattening and detachment
Macroscopic findings: usually normal appearance of the colon mucosaMicroscopic findings:
Treatment:
- Anti-diarrheal medications, such as loperamide, to manage symptoms
- Anti-inflammatory medications, such as budesonide, to reduce inflammation
- Immunosuppressants, such as azathioprine, in severe cases
- Dietary changes, such as avoiding caffeine and lactose, to help manage symptoms
Ischemic Colitis
Ischemic colitis is a condition characterized by reduced blood flow to the colon, leading to inflammation and injury of the colonic tissue. It typically occurs in older adults and is often associated with underlying vascular diseases, such as atherosclerosis or heart disease. The reduced blood flow can result from a variety of factors, including blood clots, low blood pressure, or narrowing of the blood vessels.
Causes:
- Atherosclerosis
- Blood clots
- Low blood pressure
- Vasculitis
Symptoms:
- Abdominal pain, often sudden and severe
- Bloody diarrhea
- Urgent need to defecate
Diagnosis:
- Clinical evaluation: assessment of symptoms and medical history
-
Colonoscopy with biopsy: to visualize the affected areas and
obtain tissue samples.
- Mucosal edema and erythema
- Ulcerations and hemorrhages
- Segmental involvement of the colon
- Mucosal and submucosal hemorrhage
- Coagulative necrosis of the mucosa
- Inflammatory cell infiltration
- Atrophic crypts
Macroscopic findings:Microscopic findings:
Treatment:
- Supportive care, including hydration and bowel rest
- Addressing underlying causes, such as managing blood pressure or treating vascular diseases
- Surgery in severe cases where damaged portions of the colon may need to be removed
Volvulus
Volvulus is a medical condition characterized by the twisting of a portion of the colon around its mesentery, which can lead to bowel obstruction and compromised blood flow to the affected segment. This condition can occur in various parts of the colon, but it most commonly affects the sigmoid colon and the cecum. Volvulus can occur at any age, but it is more prevalent in older adults and individuals with certain risk factors, such as chronic constipation, a history of abdominal surgery, or anatomical abnormalities of the colon.
Causes:
- Chronic constipation, this can lead to increased pressure within the colon, making it more susceptible to twisting.
- Earlier abdominal surgery can cause adhesions or scar tissue that may contribute to volvulus.
- Anatomical abnormalities, such as a redundant sigmoid colon or malrotation
- Neurological disorders, such as Parkinson's disease or multiple sclerosis as they can affect bowel motility by disrupting the normal nerve signals that control muscle contractions in the colon.
Symptoms:
- Abdominal pain and distension
- Constipation or obstipation
- Nausea and vomiting
Diagnosis:
- Clinical evaluation: assessment of symptoms and medical history. Will reveal abdominal distension and tenderness, as well as signs of bowel obstruction.
- Imaging studies: abdominal X-rays or CT scans to visualize the twisted segment of the colon and assess for bowel obstruction.
Treatment:
- Endoscopic decompression: in some cases, a flexible sigmoidoscope or colonoscope can be used to untwist the volvulus and relieve the obstruction.
- Surgery: in cases where endoscopic decompression is unsuccessful or if there are signs of bowel ischemia or perforation, surgical intervention may be necessary to remove the affected segment of the colon.
- Supportive care: including hydration, pain management, and correction of electrolyte imbalances.
Colonic Polyps
Colonic polyps are growths that form on the inner lining of the colon (large intestine). They can vary in size and shape and are classified into two main types: neoplastic polyps (which have the potential to become cancerous) and non-neoplastic polyps (which are generally benign and do not have the potential to become cancerous). The most common types of colonic polyps include:- Size: can range from a few millimeters to several centimeters
- Shape: can be pedunculated (on a stalk) or sessile (flat)
- Surface: may appear smooth or lobulated
-
Varying degrees of dysplasia:
the nuclei of the cells lining the glands may appear
enlarged, hyperchromatic (darker staining), and stratified
(layered), indicating abnormal cell growth as well as
increased rate of mitosis and a decreased amount of mucin
production. Dysplasia can be classified as low-grade or high-grade based on
the severity of the abnormalities, and is a key feature in
determining the potential for malignancy.
- Low-grade dysplasia: characterized by mild to moderate architectural and cytological abnormalities, with cells that still resemble normal glandular cells but show some irregularities in size, shape, and organization.
- High-grade dysplasia: characterized by more pronounced architectural distortion and cytological abnormalities, with cells that appear more atypical and less like normal glandular cells. High-grade dysplasia is considered a precancerous condition and has a higher risk of progressing to invasive cancer if left untreated.
- There are three main types of adenomas based on their histological features:
- Tubular adenomas: composed mainly of tubular glands (>75%); lower risk of malignancy
- Villous adenomas: composed mainly of villous structures (>75%); higher risk of malignancy
- Tubulovillous adenomas: contain both tubular and villous features; intermediate risk of malignancy
- Small size, usually less than 5 mm in diameter
- Smooth, dome-shaped appearance
- Located primarily in the distal colon and rectum
- Elongated, saw-tooth appearance of the crypts
- Increased number of goblet cells
- No dysplasia (abnormal cell growth)
- Variable size and shape
- Often found in areas of previous inflammation
- May have a friable or ulcerated surface
- Inflammatory cell infiltrate in the lamina propria
- Ulceration and granulation tissue formation
- No dysplasia (abnormal cell growth)
- Variable size and shape
- Often pedunculated (on a stalk)
- May have a lobulated surface
- Disorganized arrangement of normal tissue components
- Presence of smooth muscle, glands, and connective tissue
- No dysplasia (abnormal cell growth)
- Variable size and shape
- Often sessile (flat) or slightly elevated
- Located primarily in the proximal colon
- Saw-tooth appearance of the crypts
- Architectural distortion of the crypts
- Varying degrees of dysplasia, particularly in sessile serrated adenomas
Adenomatous polyps (adenomas):
These are neoplastic polyps that have the potential to develop into
colorectal cancer over time. They are further classified into tubular,
villous, or tubulovillous adenomas based on their histological
features.
-
Macroscopic features:
-
Histological features:
Hyperplastic polyps:
-
These are non-neoplastic polyps that are generally benign and do not
have the potential to become cancerous. They are usually small and
found in the distal colon and rectum.
-
Macroscopic features:
-
Histological features:
Inflammatory polyps:
-
These are non-neoplastic polyps that can develop as a result of
chronic inflammation in conditions such as ulcerative colitis or
Crohn's disease. They are usually benign and do not have the
potential to become cancerous.
-
Macroscopic features:
-
Histological features:
Hamartomatous polyps:
-
These are non-neoplastic polyps that are made up of an abnormal
mixture of tissue types. They are often associated with genetic
syndromes such as Peutz-Jeghers syndrome and juvenile polyposis
syndrome.
-
Macroscopic features:
-
Histological features:
Serrated polyps:
-
These polyps have a saw-tooth appearance of the crypts and can be
classified into hyperplastic polyps, sessile serrated adenomas, and
traditional serrated adenomas. Some serrated polyps, particularly
sessile serrated adenomas, have the potential to develop into
colorectal cancer.
-
Macroscopic features:
-
Histological features:
Symptoms:
- Often asymptomatic
- Rectal bleeding
- Changes in bowel habits
- Abdominal pain (if large)
Diagnosis:
- Colonoscopy with polyp removal and biopsy
- Histological examination of the removed polyps
Treatment:
Colonic polyps are often asymptomatic and are usually discovered during
routine screening procedures such as colonoscopy. However, larger polyps
may cause symptoms such as rectal bleeding, changes in bowel habits, or
abdominal pain. - Polypectomy during colonoscopy
- Regular surveillance colonoscopies
Because some types of colonic polyps have the potential to develop into colorectal cancer, it is important to remove them when they are found. This is typically done during a colonoscopy using techniques such as polypectomy (removal of the polyp using a snare or forceps). Regular surveillance colonoscopies are recommended for individuals with a history of colonic polyps to monitor for the development of new polyps or colorectal cancer and also for those with risk factors such as a family history of colorectal cancer or certain genetic syndromes. In many countries, routine screening for colorectal cancer with colonoscopy is recommended starting at age 50 for average-risk individuals.
Hemorrhoids
Hemorrhoids, also known as piles, are swollen and inflamed veins in the rectum and anus that cause discomfort and bleeding. They can be classified into two main types: internal hemorrhoids, which occur inside the anus, and external hemorrhoids, which occur under the skin around the anus.Hemorrhoids are a common condition that can affect people of all ages, but they are more prevalent in adults aged 45 to 65 years. Risk factors
- Chronic constipation or diarrhea, because of straining during bowel movements which increases pressure on the veins in the rectal area.
- Sitting for long periods of time on the toilet, which can lead to increased pressure on the rectal veins.
- Obesity, which increases pressure on the pelvic veins.
- Pregnancy, due to increased pressure on the pelvic veins from the growing uterus.
- A low-fiber diet, which can lead to constipation and straining during bowel movements.
Symptoms:
Internal hemorrhoids:
Internal hemorrhoids:
- Painless rectal bleeding during bowel movements, typically bright red blood on the toilet paper or in the toilet bowl, not mixed with the stool, and usually the amount of blood is small.
- Sensation of incomplete evacuation after a bowel movement
- Prolapse of hemorrhoids outside the anus, which may cause discomfort
- Pain or discomfort, especially during bowel movements
- Itching or irritation in the anal region
- Swelling around the anus
- A lump near the anus, which may be sensitive or painful
Diagnosis:
- Physical examination: visual inspection of the anal area for external hemorrhoids.
- Digital rectal examination: to feel for internal hemorrhoids or other abnormalities.
- Anoscopy or sigmoidoscopy: to visualize internal hemorrhoids and assess their severity.
Treatment:
- Lifestyle changes: increasing fiber intake, drinking plenty of fluids, and avoiding straining during bowel movements.
- Topical treatments: over-the-counter creams, ointments, or suppositories to relieve symptoms, such as hydrocortisone, witch hazel or lidocaine.
- Warm sitz baths: soaking the anal area in warm water to reduce discomfort.
-
Minimally invasive procedures:
- Rubber band ligation: a rubber band is placed around the base of the hemorrhoid to cut off its blood supply, causing it to shrink and fall off.
- Sclerotherapy: a chemical solution is injected into the hemorrhoid, causing it to shrink.
- Infrared coagulation: a special device is used to apply infrared light to the hemorrhoid, causing it to shrink.
-
Advanced procedures:
- Hemorrhoidectomy: surgical removal of hemorrhoids, usually reserved for severe cases or when other treatments have failed.
- Stapled hemorrhoidopexy: a surgical procedure that uses a circular stapling device to remove a ring of tissue above the hemorrhoids, which reduces blood flow to the hemorrhoids and causes them to shrink.
Anal fissures
An anal fissure is a small tear or crack in the lining of the anus, which can cause pain and bleeding during bowel movements. Anal fissures are a common condition that can affect people of all ages, but they are more prevalent in young adults and middle-aged individuals.
Causes:
- Passing large or hard stools
- Chronic constipation or diarrhea
- Straining during bowel movements
- Childbirth
- Inflammatory bowel disease
Symptoms:
- Pain during and after bowel movements
- Bright red blood on the toilet paper or in the toilet bowl
- Itching or irritation around the anus
- A visible tear or crack in the skin around the anus
Diagnosis:
- Physical examination: visual inspection of the anal area to identify the fissure.
- Digital rectal examination: to assess for any underlying abnormalities.
Treatment:
- Lifestyle changes: increasing fiber intake, drinking plenty of fluids, and avoiding straining during bowel movements.
- Topical treatments: over-the-counter creams or ointments to relieve symptoms, such as nitroglycerin, nifedipine, or lidocaine.
- Warm sitz baths: soaking the anal area in warm water to reduce discomfort.
- Botulinum toxin injections: to relax the anal sphincter muscle and promote healing.
- Surgery: in severe cases or when other treatments have failed, a lateral internal sphincterotomy may be performed to relieve pressure on the fissure and promote healing.
Proctitis
Proctitis is an inflammation of the lining of the rectum, which can cause symptoms such as rectal pain, bleeding, and diarrhea. Proctitis can be caused by a variety of factors, including infections, inflammatory bowel disease, radiation therapy, and certain medications, such as antibiotics (e.g., penicillin and amoxicillin) or nonsteroidal anti-inflammatory drugs (NSAIDs) as it can disrupt the normal balance of bacteria in the gut and lead to inflammation.
Causes:
- Infections (bacterial (e.g., sexually transmitted infections such as gonorrhea or chlamydia ), viral (e.g., herpes simplex virus or cytomegalovirus), or parasitic(e.g., Entamoeba histolytica or Giardia lamblia))
- Inflammatory bowel disease (ulcerative colitis or Crohn's disease)
- Radiation therapy, as this can damage the lining of the rectum
- Certain medications (e.g., antibiotics, NSAIDs)
Symptoms:
- Rectal pain and discomfort
- Rectal bleeding
- Diarrhea
- Urgent need to defecate
Diagnosis:
- Clinical evaluation: assessment of symptoms and medical history.
- Sigmoidoscopy or colonoscopy with biopsy: to visualize the affected areas and obtain tissue samples.
- Stool tests: to identify any infectious causes.
Treatment:
- Antibiotics or antiviral medications for infectious causes.
- Anti-inflammatory medications, such as aminosalicylates or corticosteroids.
- Immunosuppressants for inflammatory bowel disease-related proctitis.
- Supportive care, including hydration and dietary modifications.