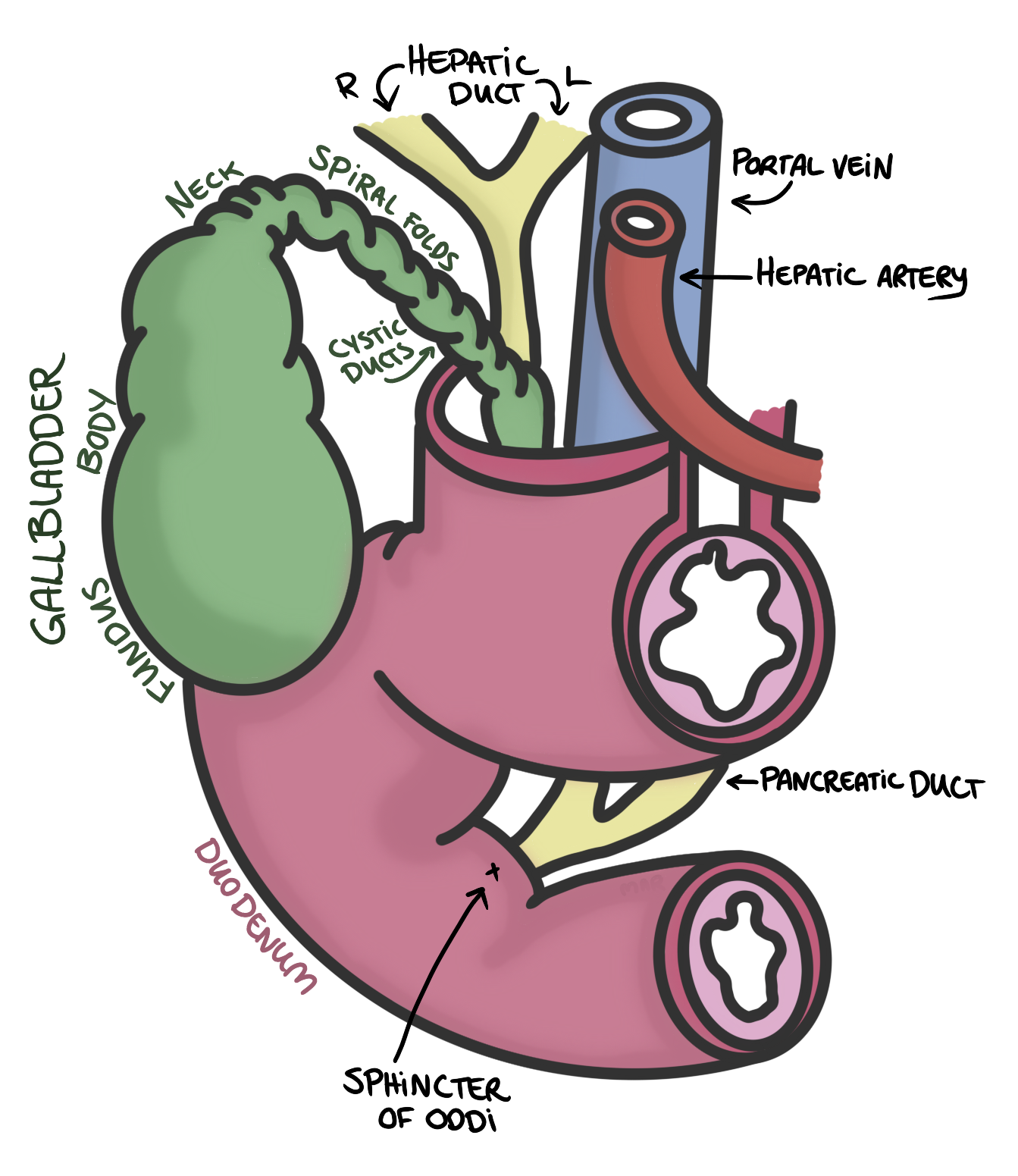
Gallbladder
Stores and concentrates bile from the liver. It releases bile into the duodenum via the common bile duct to aid in the digestion of fats.It is located on the underside of the liver and has three main parts:
Blood supply:
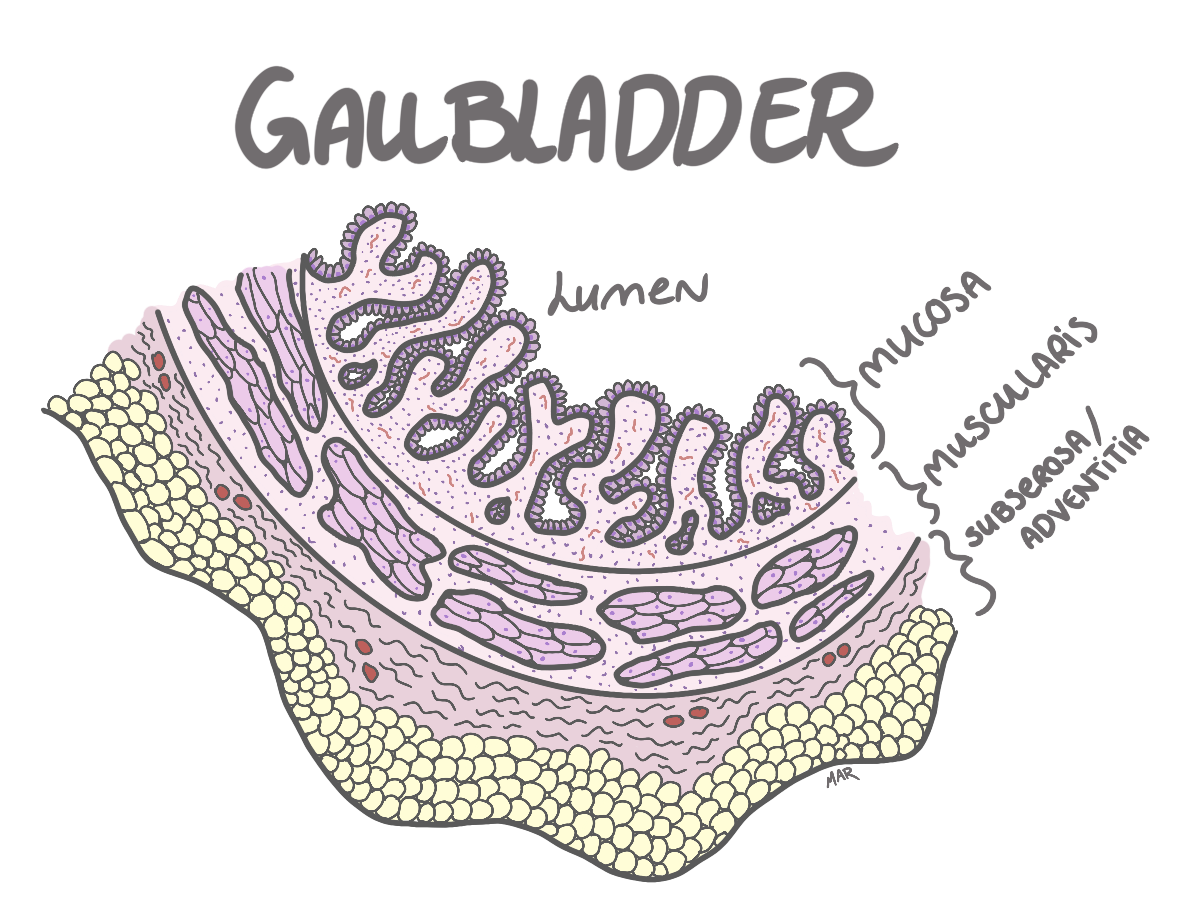
Histology
The gallbladder wall is composed of four main layers:
-
Mucosa:
Microvilli that are folded into rugae to increase surface area
for absorption, and lined by simple columnar epithelium.
Beneath the epithelium is the lamina propria, which contains
connective tissue, blood vessels, and lymphatics.
-
Muscularis Mucosa:
Thin layer of smooth muscle.
-
Subserosa/Adventitia:
Connective tissue with blood vessels and nerves.
-
Serosa:
Outer layer of connective tissue covered by mesothelium.
Pathology
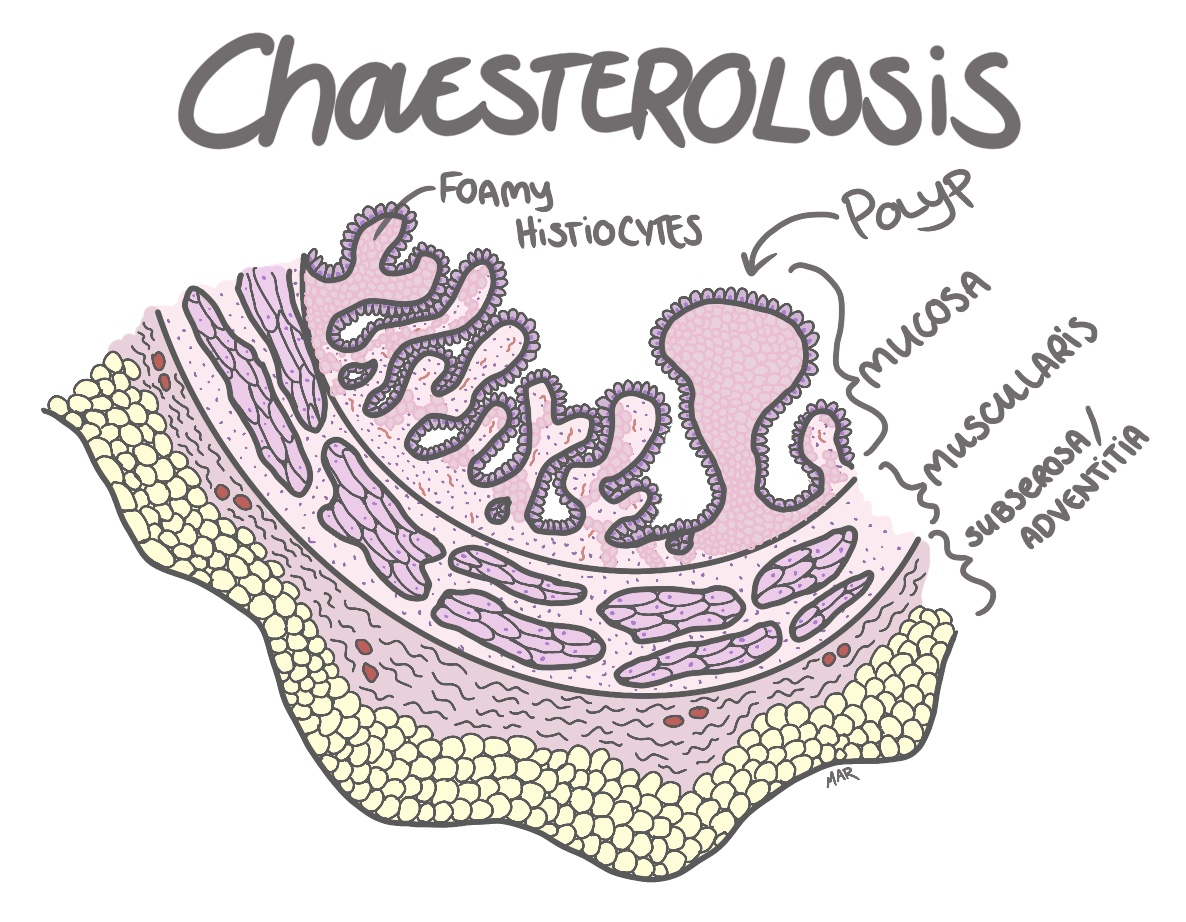
Cholesterolosis
Is when lipid accumulates in the walls of the gallbladder. Macrophages in the lamina propria then eat this lipid, turning them into foamy histiocytes (macrophages with cytoplasm filled with tiny coarse vacuoles). When there is a massiv accumulation of them sometimes polyps form, just a polypoid extrution of the lamina propria with these foamy little fellows.- Most often asymptomatic and therefore often just diagnosed incidentally during imaging or surgery
-
However, when symptomatic, it may present with:
- Biliary colic ( intermittent right upper quadrant pain after fatty meals)
- Right upper quadrant discomfort
-
Symptoms:
-
Diagnosis:
is typically made incidentally during imaging studies
(ultrasound, CT scan) or histological examination after
cholecystectomy.
-
Treatment:
usually not necessary unless symptomatic, in which case
cholecystectomy (removal of the gallbladder) may be performed.
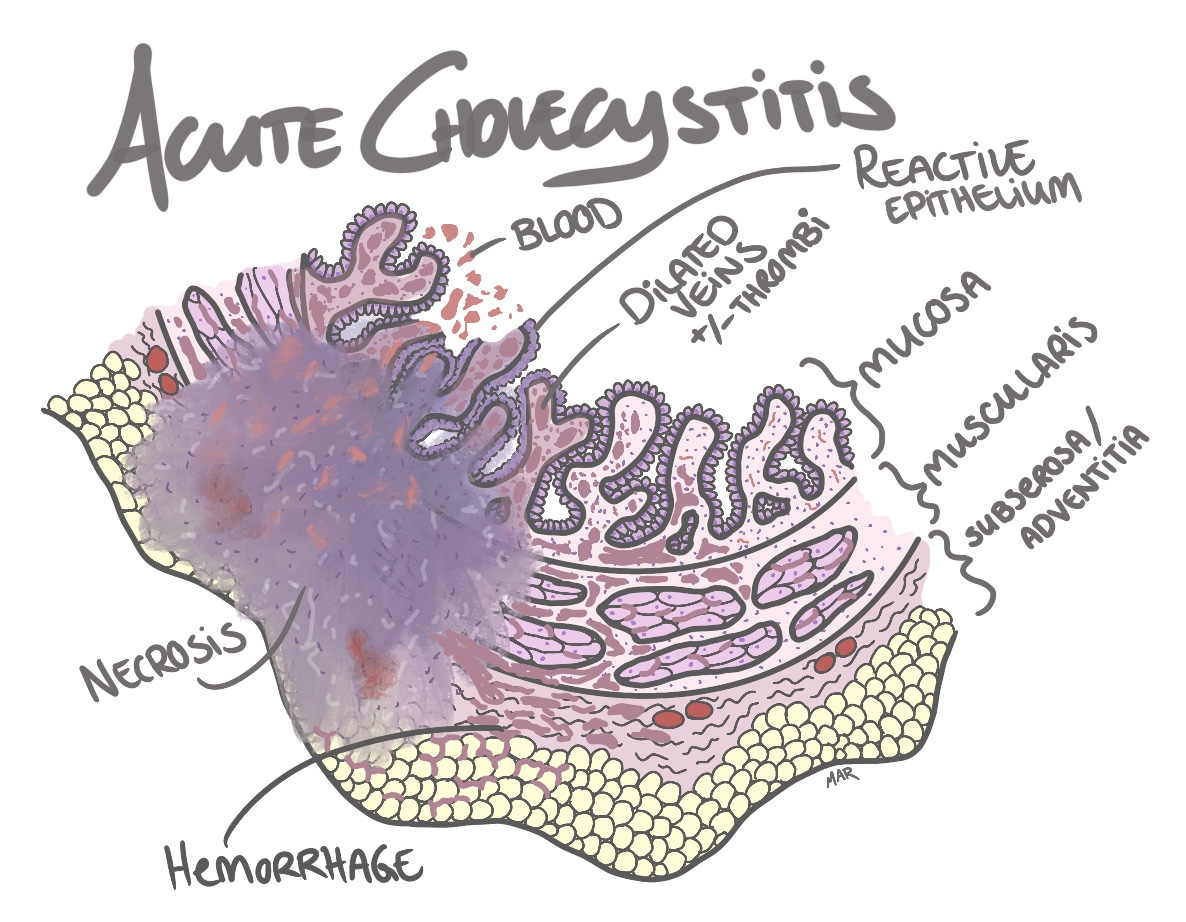
Acute cholecystitis
Is caused by blockage of the cystic duct, which is most often
caused by stones but can also be caused by a tumor or even cocaine
induced, though rare. This blockage of bile fluid can lead to
inflammation and with time edema, which in turn can to vascular
insufficiency which leads to wall ishemia and necrosis.
Microscopically you will see
edema and bleeding within the walls in combination
with necrosis. At this stage you might see
neutrofils in walls of the gallbladder. As this blockage of
bile fluid leads to increased pressure within the gallbladder,
that leads to stasis within veins, that leads to
thombi formation in the small veins, which can even lead to
fibrinoid necrosis. Sometimes gas-forming bacteria might
infect the walls and cause air-bubbles, leading to
emphysematous cholecystitis.
- sudden onset of severe right upper quadrant abdominal pain
- fever
- nausea and vomiting
- positive Murphy's sign (inspiratory arrest during deep palpation of the right upper quadrant)
- Blood test: elevated white blood cell count (leukocytosis) and elevated liver function tests (ALT, AST, ALP, bilirubin).
- Imaging: ultrasound is the preferred initial imaging modality, which may show gallstones, gallbladder wall thickening, pericholecystic fluid (fluid around the gallbladder), and a positive sonographic Murphy's sign ( maximal tenderness when the ultrasound probe is pressed over the gallbladder). A HIDA scan (a hepatobiliary iminodiacetic acid scan, radioactive tracer is used) may be performed if the diagnosis is uncertain, which will show non-visualization of the gallbladder due to cystic duct obstruction.
- supportive care with fluids and pain management
- antibiotics to cover common pathogens (often enteric bacteria, such as Escherichia coli, Klebsiella, and Enterococcus)
- surgical intervention (cholecystectomy) is often required, either urgently or electively after the acute inflammation has resolved. Most often performed laparoscopically.
-
Symptoms:
-
Diagnosis:
-
Treatment:
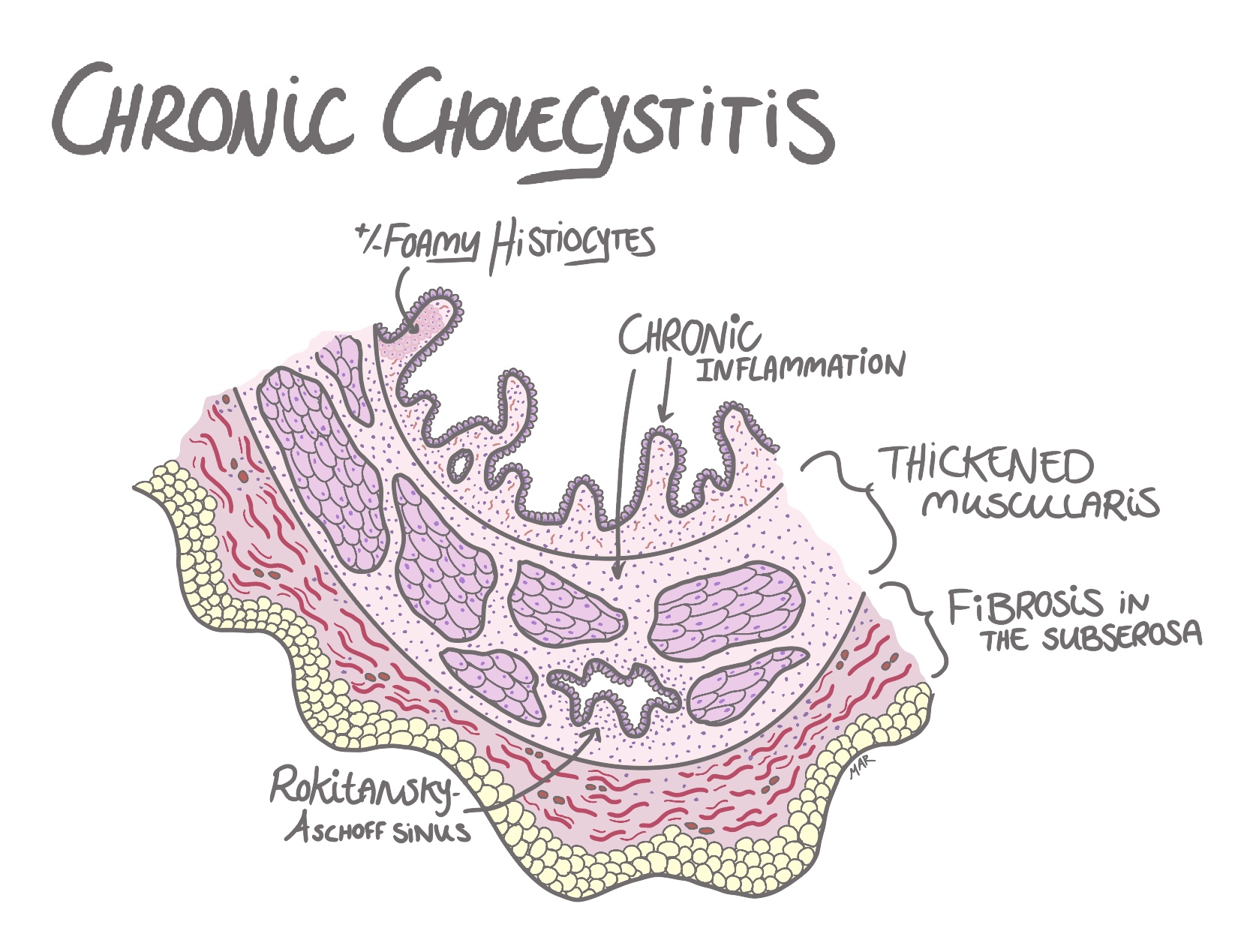
Chronic cholecystitis
Most often caused by gallstones, that leads to hyperkinesia.
Hyperkinesia then leads to
thickened muscularis (hypertrophy of the muscles),
chronic inflammation and fibrosis in the subserosa.
As gallstones are most often caused by increase biliary secreation
of cholesterol, sometimes foamy histiocyte are formed in
the lamina propria, which is a histiocytes (macrophage) with
cytoplasm filled with tiny coarse vacuoles. You will also see
Rokitansky-Aschoff sinuses, which are invaginations or
protrusions of the gallbladder epithelia that can reach the either
perimuscular or the subserosal connective tissue. This is caused
by increased luminal pressure in the gallbladder and weakened
muscular layer.
- often asymptomatic and discovered incidentally during imaging or surgery
- when symptomatic, it may present with biliary colic ( intermittent right upper quadrant pain after fatty meals)
- Blood tests: usually normal, but may show mildly elevated liver function tests (ALT, AST, ALP, bilirubin) during episodes of biliary colic.
- Imaging: ultrasound may show gallstones, gallbladder wall thickening, and a contracted gallbladder (due to chronic inflammation and fibrosis).
- Asymptomatic cases: usually do not require treatment.
-
Symptomatic cases:
-
=> dietary modifications to avoid fatty foods that can
trigger biliary colic
-
=> elective cholecystectomy (removal of the
gallbladder), if dietary modifications are insufficient
to control symptoms.
-
Symptoms:
-
Diagnosis:
-
Treatment: