Arteries & Veins
Arteries
-
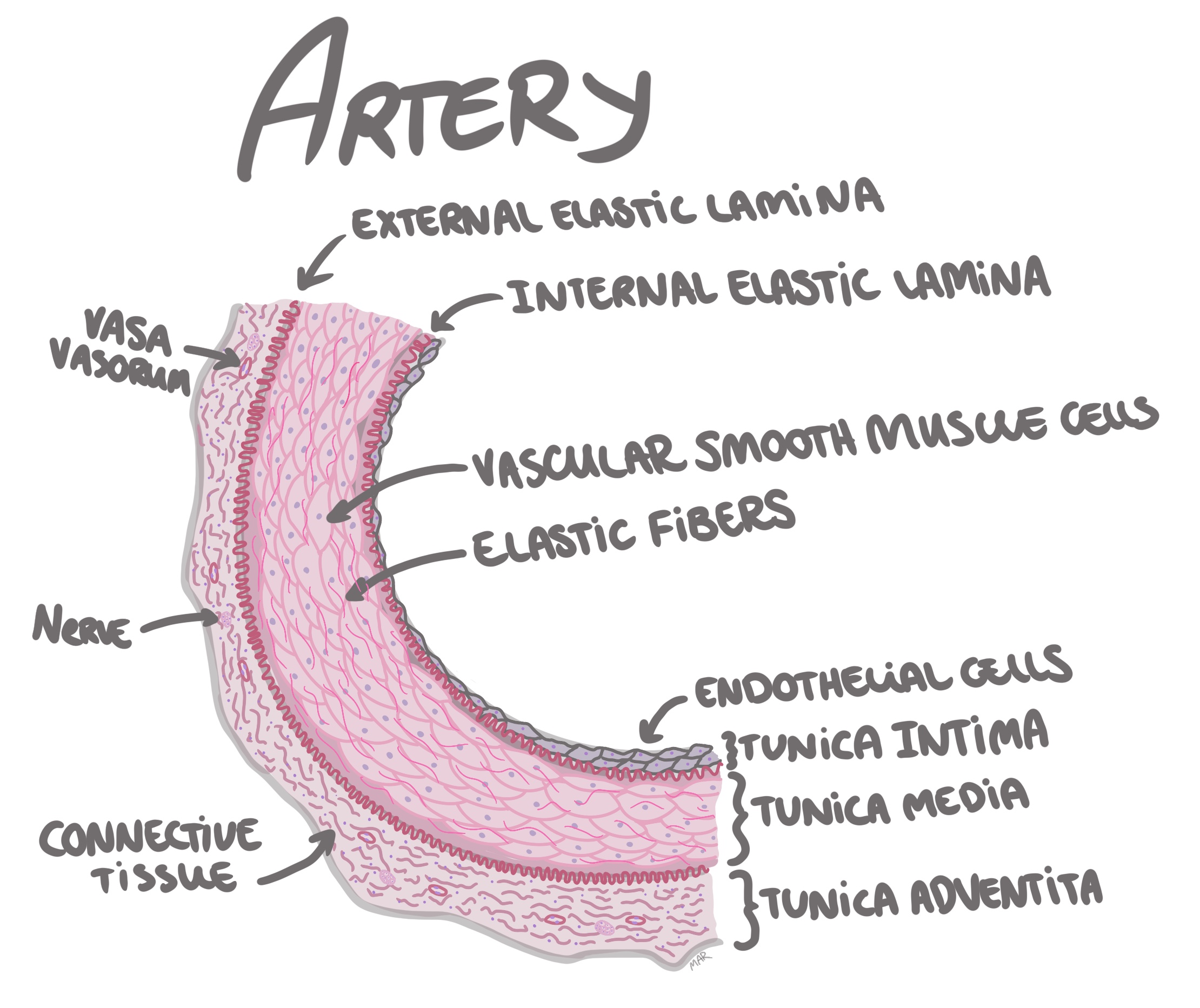
Tunica intima
the inner layer of the artery, composed of endothelial cells,
underlying loose connective tissue and internal elastic lamina
(elastic membrane) that seperates tunica intima from tunica
media. The endothelial cells tend to proliferate as response to
injury (altered blood flow or increased pressure). This layer is
affected by progressive intimal fiborsis, that is especially
prominent in the thyroid, spleen and myometrium.
-
Tunica media
the middle layer of the artery, composed of vascular smooth
muscle cells, elastic tissue and collagen.
-
Tunica adventitia
it the outer most layer, composed mostly of collagen fibers,
elastic fibers and fibroblasts. You might also see macrophages
and other inflammatory cells, ganglion cells and vasa vasorum
(small blood vessels that supply the larger ones).
Infarction of the myocardium - coronary arteries
Timeline
-
0h
coronary artery gets clogged.
-
4-12h
myocytes become hypereosinophilic (more pink),contraction bands
appear (hypercontraction of sarcomeres in myocytes).
-
24-48h
neutrofils appear in the interstitium. If blood flow is
reestablished, you might see abundant interstitial hemorrhage
(reperfusion damage).
-
48-72h
neutrofils start to degenerate, and therefore you have a mix og
vital and degenerating neutrofils. Close to 72h you therefore see
abundant cellular debris.
-
Day 3
mononuclear cells start dominating the picture.
-
Day 3-5
myocytes are removed and you will find lymfocytes, pigment-laden
histiocytes (macrophages) along with myofibroblasts in the
interstitium.
-
Day 5-7
The interstitial cells increase in number, but no collagen has
been produced, which is why the myocardial wall is here at its
weakest and often the time of rupture.
-
Day 7
collagen starts to appear and inflammatory cells begin to
disappear. From here on after, the age of the infarction is
dependent on the extent of the collagen and remaining
inflammation.
-
2 months
inflammation has disappeared and only collagen remains, id est a
scar is formed.
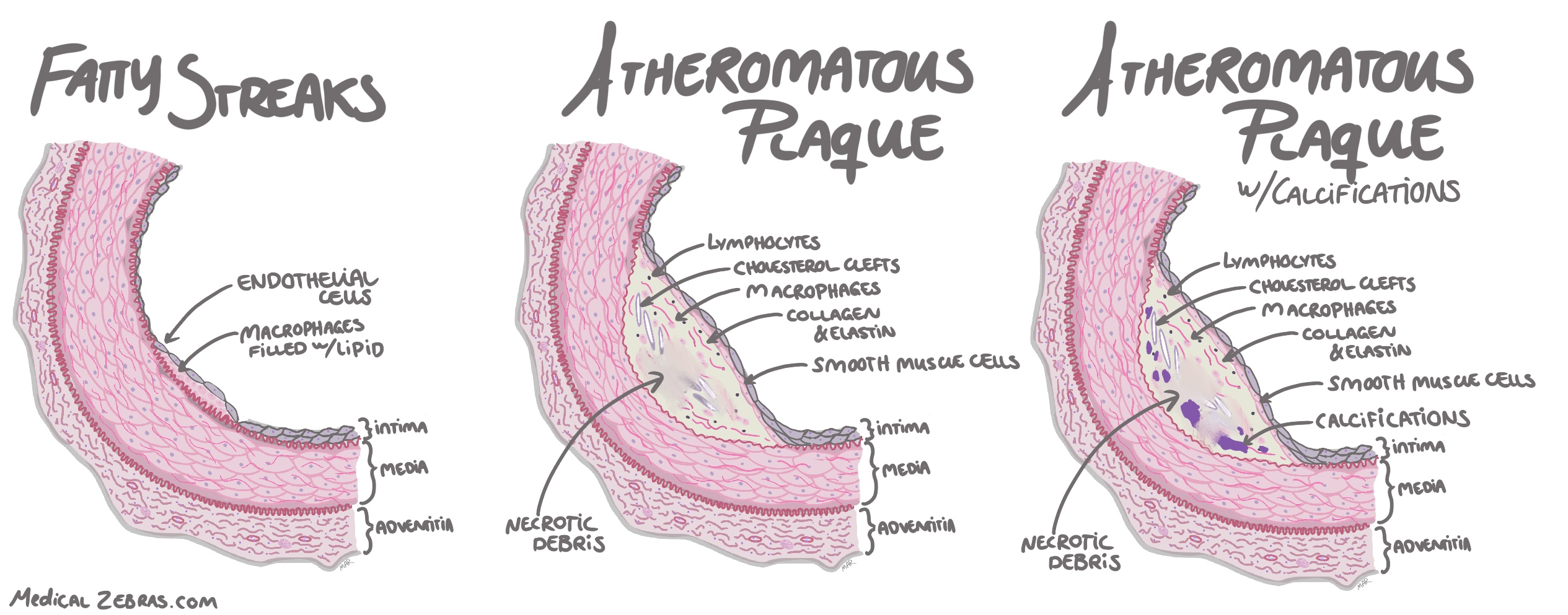
Atherosclerosis
One of the most common place for artherosclerosis is where the arteries bifurcate (split), as the bifurcation cases blood flow turbulance.
-
Fatty streaks:
a visible yellow to white lesion on the intimal surface, where
macrophages filled with lipid have accumulated beneath the
endothelium in the intima.
-
Atheromatous plaques:
are raised yellow to white lesions within the intima. The lesion
contains a lipid core and necrotic debris covered by a fibrous cap.
The fibrous cap contains smooth muscle cells, macrophages filled
with lipid, collagen and elastin as well as lymphocytes. The
necrotic center contains cellular debris, macrophages filled with
lipid, cholesterol crystals and calcium. This plaque can increase in
size with time and therefore protrude into the lumen causing
stenosis (decreased lumen) and affect the quality of the media
underneath which in some cases can lead to aneurysm formation.
-
Calcification:
As the lipid core in the atheromatous plaque contains calcium, this
accumulation with time will lead to calcifications within the
plaque. Calcium mainly comes from dying cells that leak calcium into
the extracellular matrix.
-
Stenosis:
is when the atheromatous plaque protrudes into the arterial lumen
decreasing the diameter of the lumen, thus disturbing and decreasing
blood flow.
Cardiomyopathy
Hypertrophic cardiomyopathy
Is when the heart muscle or the myocardium becomes thickened (hypertrophied). This can lead to diastolic dysfunction (the heart cannot relax normally), valves might not be able to close normally leading to regurgitation and even myocardial ischemia as the abnormal myocytes can compress small arteries in the heart. Hypertrophic cardiomyopathy can either be aquired or genetic. The acquired causes include hypertension and aortic stenosis, which both increase the pressure tension in the heart.Genetic causes include mutations in genes that encode sarcomere-associated proteins, like beta-myosin heavy chain and myosin binding protein C.
To be diagnosed with hypertrophic cardiomyopathy as an adults the left ventricular end diastolic wall thickness should be >13 mm or > 15 mm (on imaging) depending on criteria used.
Histology
Dilated cardiomyopathy
Is when the heart ventricles, one or both, have enlarged, and the myocardium stretched and thinned, leading to impaired contraction (left ventricular ejection fraction, LVEF, under 40%).Histology