Anatomy, histology and physiology
The heart is a muscular organ the size of a fist (about 12 cm long
and 8-9 cm wide, weighing between 250-350 grams in adults) that
pumps blood through the blood vessels of the circulatory system.
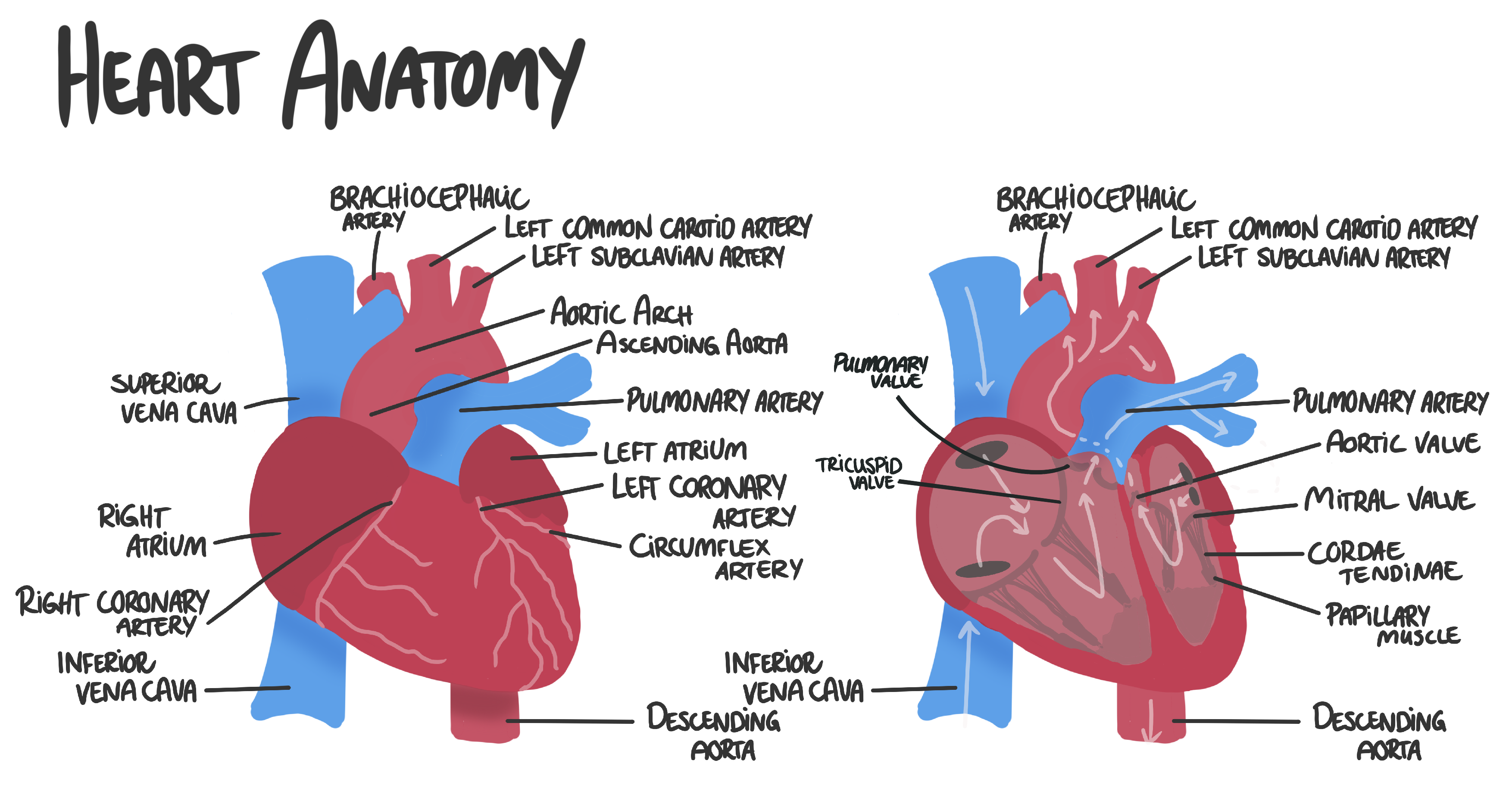
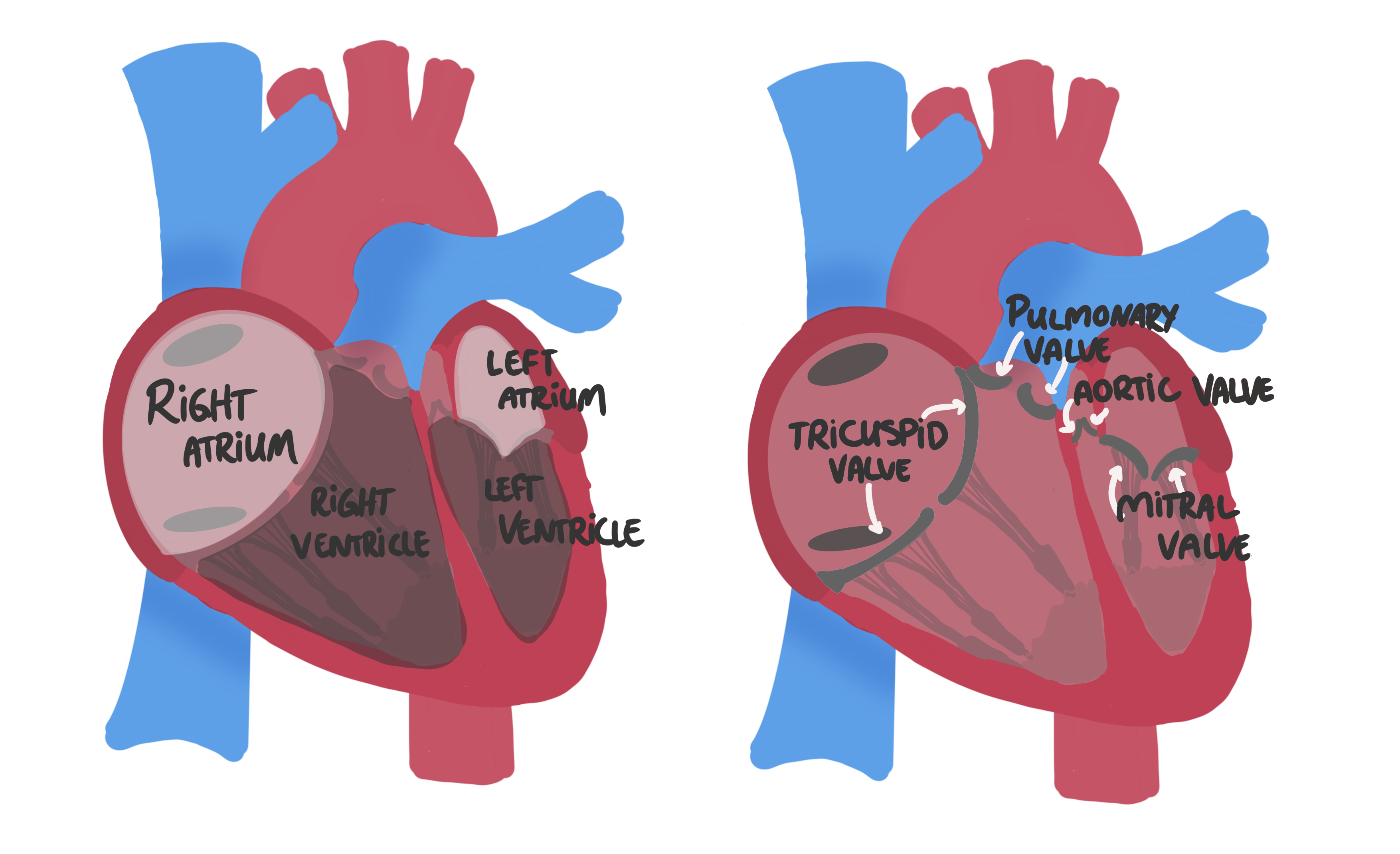
The heart has four chambers: two atria (upper chambers) and two ventricles (lower chambers). The right side of the heart receives deoxygenated blood from the body and pumps it to the lungs for oxygenation, while the left side receives oxygenated blood from the lungs and pumps it to the rest of the body.
The heart has four main valves that regulate blood flow between the chambers and prevent backflow:
The heart has four chambers: two atria (upper chambers) and two ventricles (lower chambers). The right side of the heart receives deoxygenated blood from the body and pumps it to the lungs for oxygenation, while the left side receives oxygenated blood from the lungs and pumps it to the rest of the body.
The heart has four main valves that regulate blood flow between the chambers and prevent backflow:
-
Tricuspid valve: between the right atrium and right ventricle.
-
Pulmonary valve: between the right ventricle and pulmonary artery
-
Mitral valve: between the left atrium and left ventricle
-
Aortic valve: between the left ventricle and aorta
-
Left coronary artery
supplies blood to the left atrium, left ventricle, and
interventricular septum.
-
Left anterior descending artery (LAD)
supplies blood to the anterior wall of the left ventricle and
the interventricular septum.
-
Left circumflex artery
supplies blood to the lateral and posterior walls of the left
ventricle.
-
Right coronary artery
supplies blood to the right atrium, right ventricle, and
inferior wall of the left ventricle.
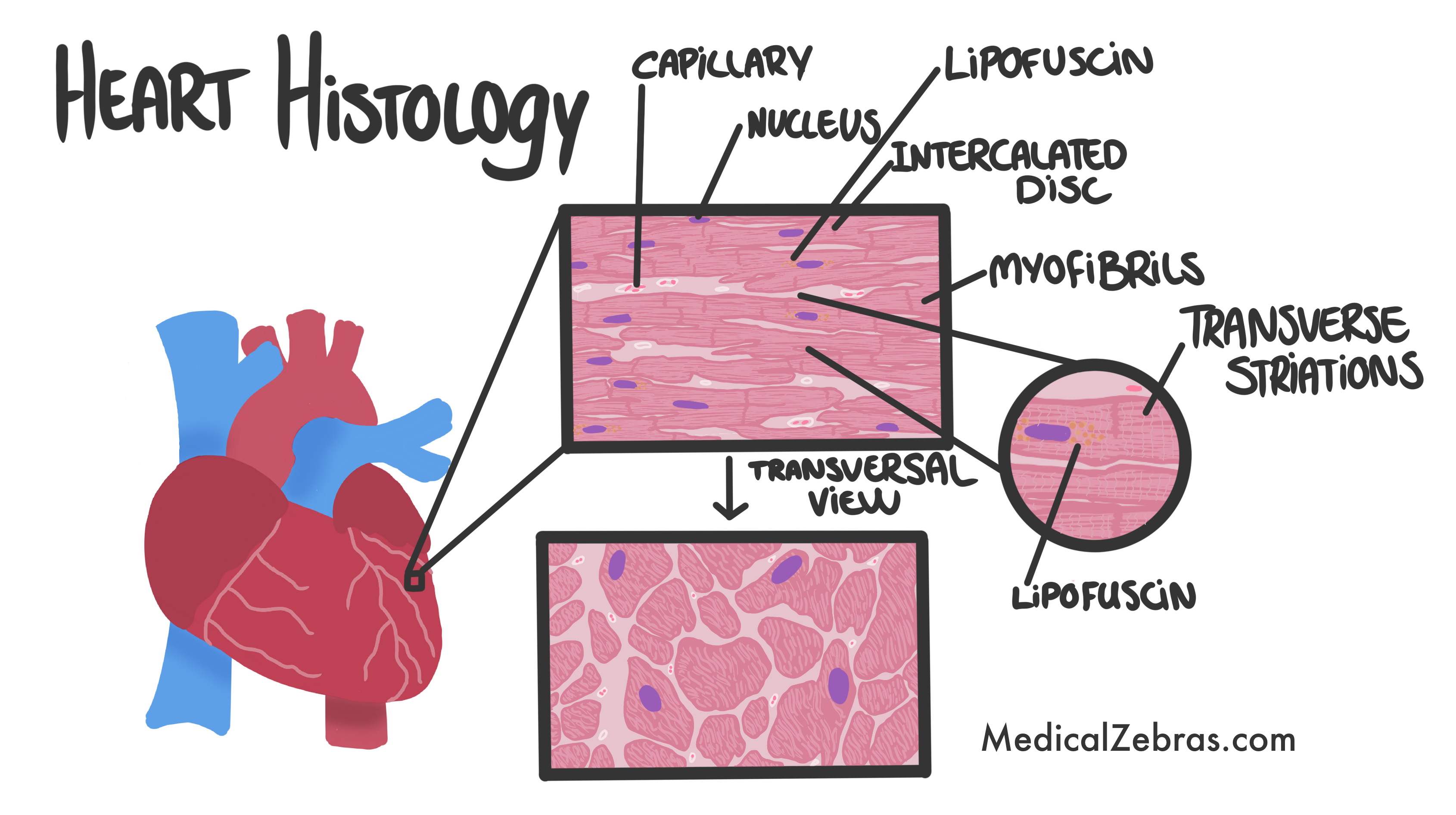
The heart wall consists of three layers:
- Endocardium: The innermost layer that lines the heart chambers and valves. It is composed of endothelial cells and connective tissue.
- Myocardium: The middle layer that contains the cardiac muscle cells, called cardiomyocytes, responsible for the heart's contractile function. These cells are striated, and connected via intercalated discs which are essential for synchronized contraction of the heart muscle. Cardiomyocytes have a high density of mitochondria to meet the energy demands of continuous contraction. With time and as we age, within some cardiomyocytes, there is an accumulation of oxidized lipids and proteins called lipofuscin a yellowish-brown pigment. This is a normal part of aging and is often referred to as the "wear and tear" pigment.
- Epicardium: The outermost layer that covers the heart's surface. It is also known as the visceral layer of the pericardium and consists of connective tissue and fat.
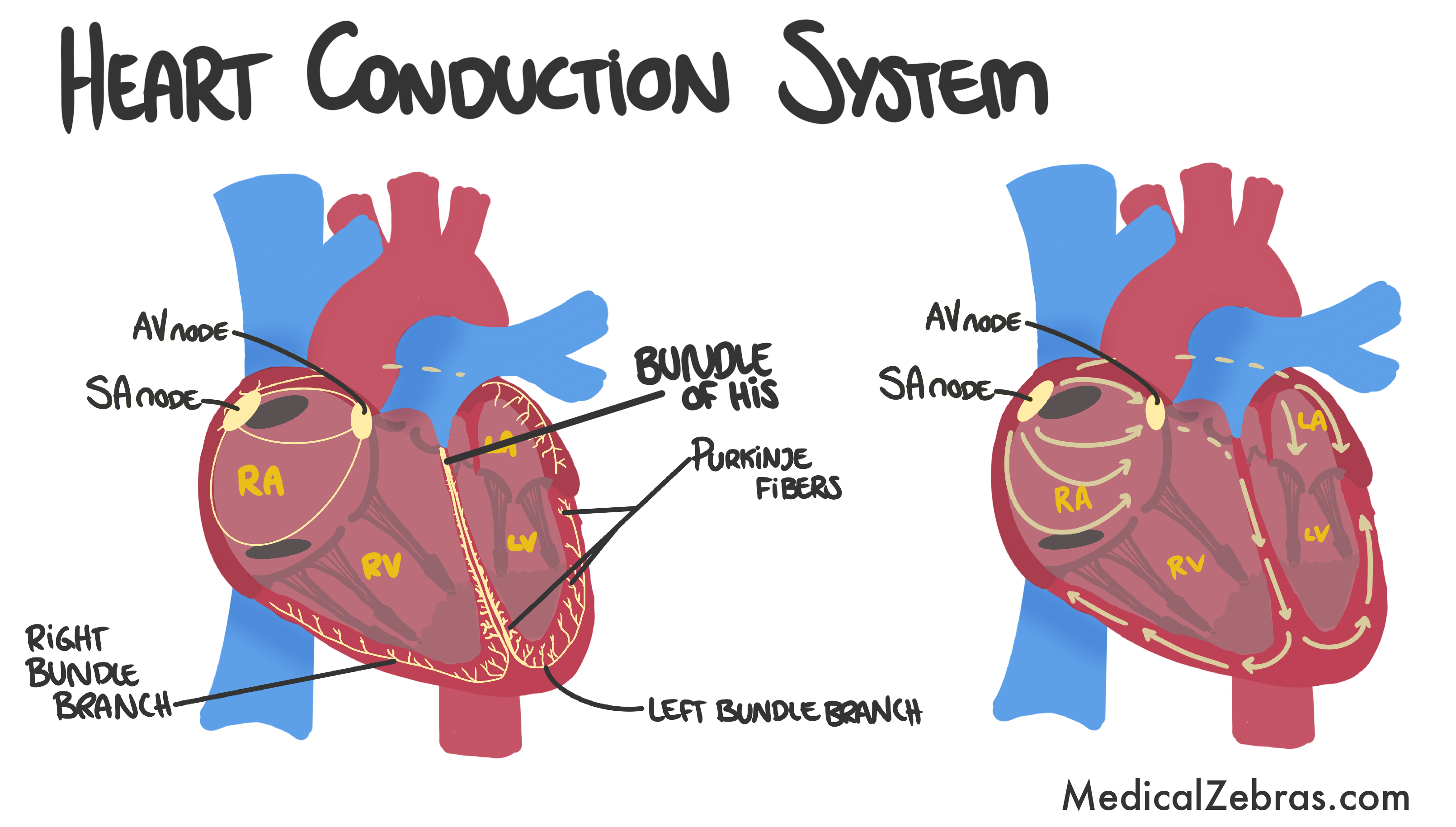
The heart has a specialized conduction system that coordinates the
heart's electrical activity and ensures that the heart beats in a
regular rhythm. The conduction system is as follows:
- Sinoatrial (SA) node: sends signal through both atriums which then ends in the AV-node.
- Atrioventricular (AV) node: sends signals to the bundle of His, but delays the signal a bit to make sure the atriums have contracted before the ventricles do.
- Bundle of His: starts where the AV-node ends and extends into the ventricles. Transfers the signal to the right and left bundle branches.
- Right and left bundle branches: runs along the interventricular septum towards the apex of the heart. Here the signal is transferred to the Purkinje fibers.
- Purkinje fibers: go from the bundle branches and into the walls of the ventricles.
ECG
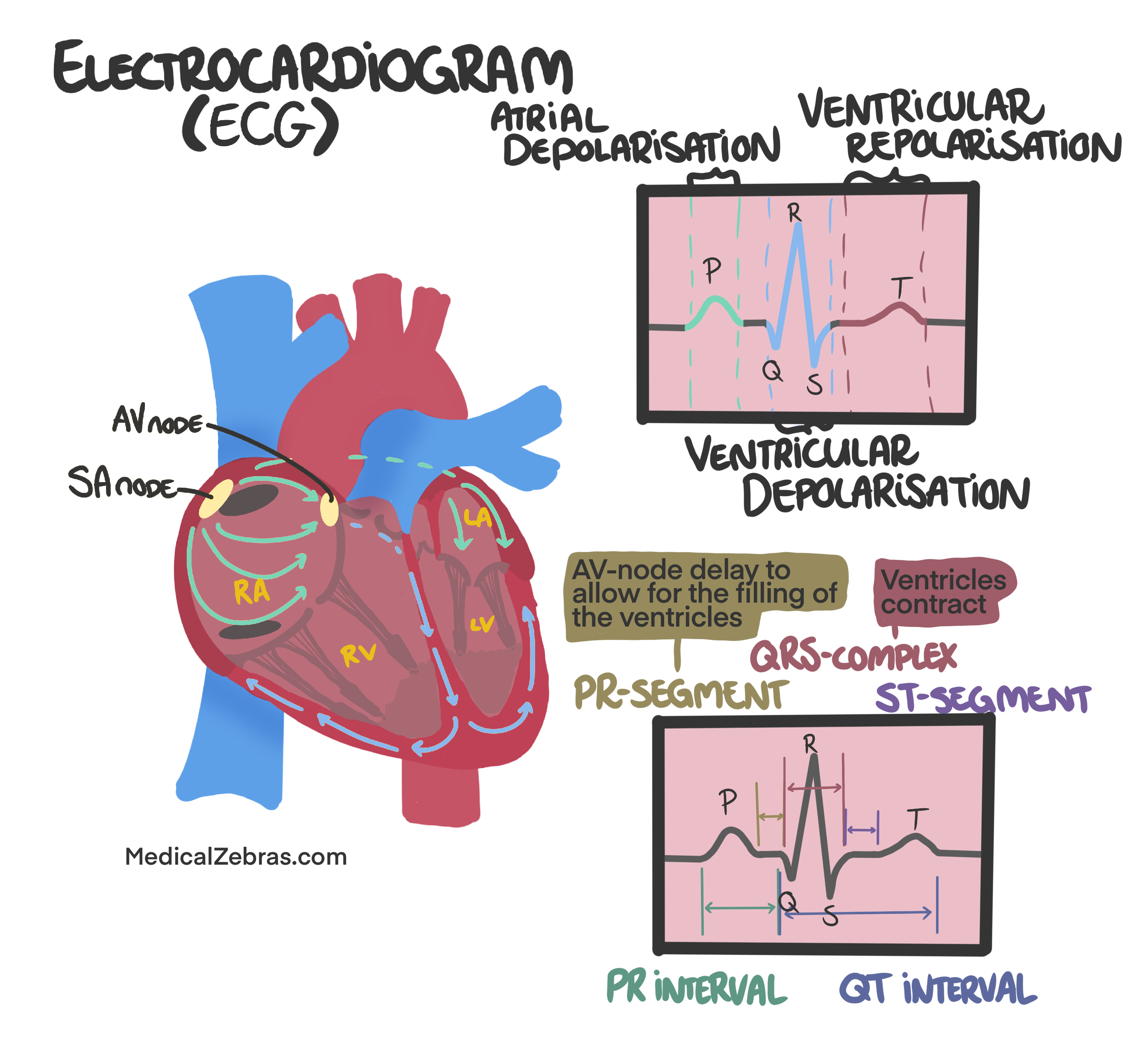
An electrocardiogram (ECG or EKG) is a test that measures the electrical activity of the heart. It is a non-invasive and painless procedure that involves placing electrodes on the skin on the left side of the chest to record the heart's electrical signals. The ECG produces a graph that shows the timing and strength of the electrical signals as they travel through the heart. The ECG can provide important information about the heart's rhythm, rate, and overall function. It can also help diagnose various heart conditions, such as arrhythmias, heart attacks, and other cardiac abnormalities. Usually to diagnose a rythm, only a few electrodes are needed, however if the goal is to pinpoint a location of, for example, an infarction or ischemia, more electrodes in more locations is needed.The main components of an ECG waveform include:
- P wave: represents atrial depolarization, which is the electrical activity that triggers atrial contraction.
- QRS complex: represents ventricular depolarization, which is the electrical activity that triggers ventricular contraction. The QRS complex is typically the largest waveform on the ECG.
- T wave: represents ventricular repolarization, which is the electrical activity that occurs as the ventricles recover from contraction and prepare for the next heartbeat.
- PR interval: the time between the start of the P wave and the start of the QRS complex. It reflects the time it takes for the electrical signal to travel from the atria to the ventricles.
- QT interval: the time between the start of the QRS complex and the end of the T wave. It reflects the time it takes for the ventricles to depolarize and repolarize.
- PR segment: represents the delay of the signal in the AV node.
-
ST segment: represents the time between ventricular
depolarization and repolarization, and is important in
diagnosing myocardial ischemia or infarction.
-
ST-elevation: indicates myocardial
injury, often due to acute myocardial infarction (heart attack).
-
ST-depression: indicates myocardial
ischemia, which can be caused by conditions such as angina or
coronary artery disease.
Pathology
Ischemic heart disease
Is a condition characterized by reduced blood flow to the heart muscle (myocardium) due to narrowing or blockage of the coronary arteries. This can lead to chest pain (angina), shortness of breath, and other symptoms. If left untreated, ischemic heart disease can lead to heart attacks and heart failure.The most common cause of ischemic heart disease is atherosclerosis, a condition in which fatty deposits (plaques) build up in the walls of the coronary arteries, leading to narrowing and reduced blood flow. Other risk factors for ischemic heart disease include high blood pressure, smoking, diabetes, obesity, and a family history of heart disease.
Clinical features
-
Stable angina: is characterized by chest pain or discomfort that occurs with
exertion or emotional stress and is
relieved by
rest or nitroglycerin. The pain is usually described as a pressure
or tightness in the chest and may radiate to the arms, neck, jaw, or
back. Stable angina is typically caused by atherosclerosis and is a
warning sign of underlying coronary artery disease.
-
Unstable angina: is characterized by chest pain or discomfort that occurs at rest
or with minimal exertion and is
not relieved
by rest or nitroglycerin. The pain may be more severe and prolonged
than stable angina and may be associated with other symptoms such as
shortness of breath, sweating, nausea, or lightheadedness. Unstable
angina is a medical emergency and requires immediate evaluation and
treatment.
-
Myocardial infarction (heart attack): occurs when a coronary artery is completely blocked, leading to
death of the affected area of the myocardium. Symptoms of a heart
attack may include chest pain (often described as a crushing or
squeezing sensation, often radiating to the left arm, neck, jaw, or
back) or discomfort that lasts for more than a few minutes,
shortness of breath, sweating, nausea, or lightheadedness. A heart
attack is a medical emergency and requires immediate evaluation and
treatment.
Diagnosis
The diagnosis of ischemic heart disease is based on a combination of clinical history, physical examination, and diagnostic tests. Common diagnostic tests include:-
Electrocardiogram (ECG or EKG): can detect changes in the heart's electrical activity that may
indicate ischemia or infarction.
-
ST elevation: indicates myocardial
injury, often due to acute myocardial infarction (heart attack).
-
ST depression: indicates myocardial
ischemia, which can be caused by conditions such as angina or coronary
artery disease.
-
Other signs include
T-wave flattening or inversion. T-wave inversions can indicate ischemia and T-wave flattening
can be a sign of ischemia as well, but is less specific.
Pathological Q waves, for example wide and deep Q wave, can indicate a previous
myocardial infarction, but can also indicate other conditions such
as cardiomyopathy or conduction abnormalities, pregnancy, or just
misplaced electrodes.
-
Stress testing: involves exercising on a treadmill or bike while monitoring the
heart's response. This can help identify areas of the heart that are
not receiving enough blood flow.
-
Echocardiography: uses sound waves to create images of the heart and can help
assess the heart's function and identify areas of damage.
-
Coronary angiography: involves injecting a contrast dye into the coronary arteries and
taking X-ray images to visualize any blockages or narrowing.
-
Blood tests: can measure levels of certain enzymes and proteins that may
indicate damage to the heart muscle, like for example
troponin, that is released when the heart muscle is damaged. BNP (B-type
natriuretic peptide) can also be measured, as it is released in
response to increased pressure in the heart and can be elevated in
heart failure.
Treatment
Treatment for ischemic heart disease may include:-
Life style changes:
such as diet (to lower cholesterol levels), smoking cessation,
weight loss and exercise (to improve cardiovascular health).
-
Medications:
such as aspirin (to reduce blood clotting) , beta-blockers (to
reduce heart rate and blood pressure) , and statins ( to lower
cholesterol levels in the blood).
-
Procedures:
such as angioplasty and stenting (to open up blocked arteries) or
coronary artery bypass surgery (to create a new route for blood flow
around blocked arteries).
Complications
Complications of ischemic heart disease may include heart failure, arrhythmias, and sudden cardiac death. If the infarct is big enough, it can lead to cardiogenic shock, which is a state of inadequate tissue perfusion due to the heart's inability to pump enough blood to meet the body's needs. This can lead to organ failure and death if not treated promptly. Also mechanical complications can occur, such as ventricular free wall rupture, interventricular septal rupture, and papillary muscle rupture, which can lead to acute mitral regurgitation. These complications are more likely to occur in the first week after a myocardial infarction, when the infarcted tissue is still weak, as scar tissue has not formed yet, and therefore the affected area is vulnerable to rupture. If a rupture occurs, it can lead to sudden death due to cardiac tamponade (blood leaks into and fills the pericardial sac that surrounds the heart, so the heart no longer has space to function) or severe mitral regurgitation.Histology
- Atherosclerosis: is characterized by the presence of fatty plaques in the walls of the coronary arteries. These plaques are made up of cholesterol, inflammatory cells, and other substances. The plaques can cause narrowing of the arteries, leading to reduced blood flow to the myocardium.
- Myocardial ischemia: is characterized by the presence of areas of the myocardium that are deprived of oxygen and nutrients due to reduced blood flow. This can lead to myocyte injury and death, as well as inflammation and fibrosis in the affected areas.
- Myocardial infarction: is characterized by the presence of areas of the myocardium that have undergone necrosis (cell death) due to prolonged ischemia. This can lead to the formation of scar tissue in the affected areas, which can impair the function of the heart.
Infarction
Most often infarctions are caused by atherosclerosis of the coronary arteries, which can lead to thrombosis and occlusion of the artery. This causes ischemia of the area supplied by the artery. The most common artery to be affected is the left anterior descending artery (LAD), which supplies the anterior wall of the left ventricle and the interventricular septum. Other arteries that can be affected include the right coronary artery (RCA) and the left circumflex artery (LCX).Histological Timeline
-
0h
coronary artery gets clogged. In the first 4 hours there are no
histologic changes.
-
4-12h
myocytes become hypereosinophilic (more pink) because of coagulative
necrosis, contraction bands appear (hypercontraction of sarcomeres
in myocytes).
-
24-48h
neutrofils appear in the interstitium. If blood flow is
reestablished, you might see abundant interstitial hemorrhage
(reperfusion damage).
-
48-72h
neutrofils start to degenerate, and therefore you have a mix og
vital and degenerating neutrofils. Close to 72h you therefore see
abundant cellular debris.
-
Day 3
mononuclear cells start dominating the picture.
-
Day 3-5
myocytes are removed and you will find lymfocytes, pigment-laden
histiocytes (macrophages) along with myofibroblasts in the
interstitium.
-
Day 5-7
The interstitial cells increase in number, but no collagen has been
produced, which is why the myocardial wall is here at its
weakest
and often the time of rupture.
-
Day 7
collagen starts to appear and inflammatory cells begin to disappear.
From here on after, the age of the infarction is dependent on the
extent of the collagen and remaining inflammation.
-
2 months
inflammation has disappeared and only collagen remains => a scar is
formed.
Heart failure
Is a condition in which the heart is unable to pump enough blood to meet the body's needs. This can lead to symptoms such as shortness of breath, fatigue, and swelling in the legs and ankles. Heart failure can be caused by a variety of factors, including coronary artery disease, high blood pressure, and cardiomyopathy.There are two main types of heart failure based on ejection fraction, which is a measure of how much blood the left ventricle pumps out with each contraction (compared to how much blood was in the ventricle before the contraction):
- Heart failure with reduced ejection fraction (HFrEF): also known as systolic heart failure, occurs when the heart's ability to contract and pump blood is impaired. This is typically defined as a left ventricular ejection fraction (LVEF) of less than 40%.
- Heart failure with preserved ejection fraction (HFpEF): also known as diastolic heart failure, occurs when the heart's ability to relax and fill with blood is impaired. This is typically defined as a left ventricular ejection fraction (LVEF) of 50% or higher, along with evidence of diastolic dysfunction.
Histology
- HFrEF: myocytes tend to have increased length with enlarged nuclei (hypertrophy). Focal myocyte death leads to fibrosis. This can lead to increased inflammation in the interstitium.
- HFpEF: myocytes tend to have increased width with enlarged nuclei (hypertrophy). There is often interstitial fibrosis present, which can lead to stiffening of the myocardium and impaired relaxation. There may also be evidence of microvascular disease, which can contribute to ischemia and myocyte injury.
Causes
Common causes of heart failure include coronary artery disease, hypertension, cardiomyopathy, valvular heart disease, and arrhythmias. Other factors that can contribute to heart failure include diabetes, obesity, and smoking.Diagnosis
The diagnosis of heart failure is based on a combination of clinical history, physical examination, and diagnostic tests. Common diagnostic tests include:-
Electrocardiogram (ECG or EKG): can detect changes in the heart's electrical activity that may
indicate underlying heart disease.
-
Echocardiography: uses sound waves to create images of the heart and can help
assess the heart's function and identify areas of damage.
-
Chest X-ray: can help identify signs of heart failure, such as an enlarged
heart or fluid in the lungs.
-
Blood tests: can measure levels of certain enzymes and proteins that may
indicate damage to the heart muscle, like for example
troponin, that is released when the heart muscle is damaged. BNP (B-type
natriuretic peptide) can also be measured, as it is released in
response to increased pressure in the heart and can be elevated in
heart failure.
Treatment
Treatment for heart failure may include:-
Life style changes:
such as fluid restriction (to decrease preload), low salt diet (to
decrease fluid retention), exercise (to improve cardiovascular
fitness and overall health).
-
Medications:
-
ACE and ARB inhibitors, such as enalapril, ramipril, candesartan, losartan, valsartan
(to reduce blood pressure and decrease afterload),
-
Beta-blockers, such as metaprolol, atenolol, propranolol, sotalol, carvedilol
(to reduce heart rate and myocardial oxygen demand),
-
Diuretics
(to reduce fluid retention)
-
Thiazide diuretics, such as hydrochlorothiazide, chlorthalidone
-
Loop diuretics, such as furosemide, bumetanide
-
Potassium-sparing diuretics (aldosterone antagonists or
sodium channel blockers) , such as spironolactone, eplerenone, amiloride
-
Vasodilators
(to reduce afterload), such as nitrates (nitroglycerin and
isosorbide mononitrate) and hydralazine
-
Nitrates:
work mainly on veins (venodilators) to reduce preload and on
coronary arteries to improve blood flow to the myocardium.
-
Hydralazine:
works mainly on arterioles (arteriodilator) to reduce afterload.
-
Inotropes
(to increase contractility), such as digoxin (a sodium- potassium
ATPase inhibitor ), dobutamine (a beta-1 agonist), and milrinone
(a phosphodiesterase-3 inhibitor ).
-
Procedures:
really depends on the underlying cause of the heart failure, but can
include procedures such as implantable devices (like pacemakers and
defibrillators), heart pumps (LVADs), and heart transplantation to
improve heart function and manage symptoms.
Cardiomyopathy
Hypertrophic cardiomyopathy
Is when the heart muscle or the myocardium becomes thickened (hypertrophied). This can lead to diastolic dysfunction (the heart cannot relax normally), valves might not be able to close normally leading to regurgitation and even myocardial ischemia as the abnormal myocytes can compress small arteries in the heart. Hypertrophic cardiomyopathy can either be aquired or genetic. The acquired causes include hypertension and aortic stenosis, which both increase the pressure tension in the heart.Genetic causes include mutations in genes that encode sarcomere-associated proteins, like beta-myosin heavy chain and myosin binding protein C.
To be diagnosed with hypertrophic cardiomyopathy as an adults the left ventricular end diastolic wall thickness should be >13 mm or > 15 mm (on imaging) depending on criteria used.
Histology
Dilated cardiomyopathy
Is when the heart ventricles, one or both, have enlarged, and the myocardium stretched and thinned, leading to impaired contraction (left ventricular ejection fraction, LVEF, under 40%).
Histology