Anatomy & Histology
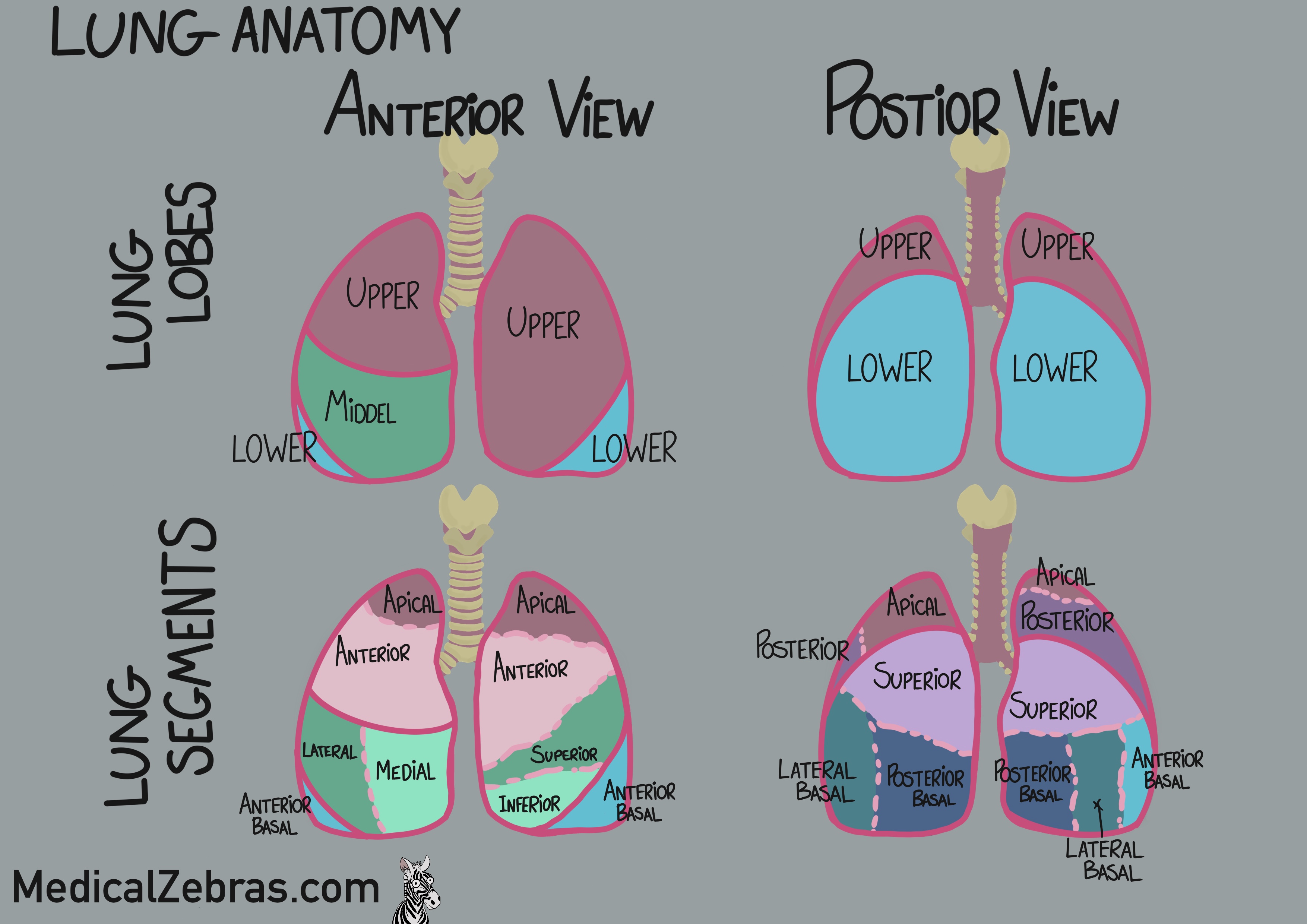
Lungs are a pair of spongy, air-filled organs located in the
thoracic cavity, responsible for gas exchange between the air we
breathe and the bloodstream. The lungs are divided into lobes, and
the lobes are further divided into segments:
-
Right lung
- Lobes: superior, middle, and inferior
- Segments: 10 in total
-
Left lung
- Lobes: superior and inferior
- Segments: 8-10 in total
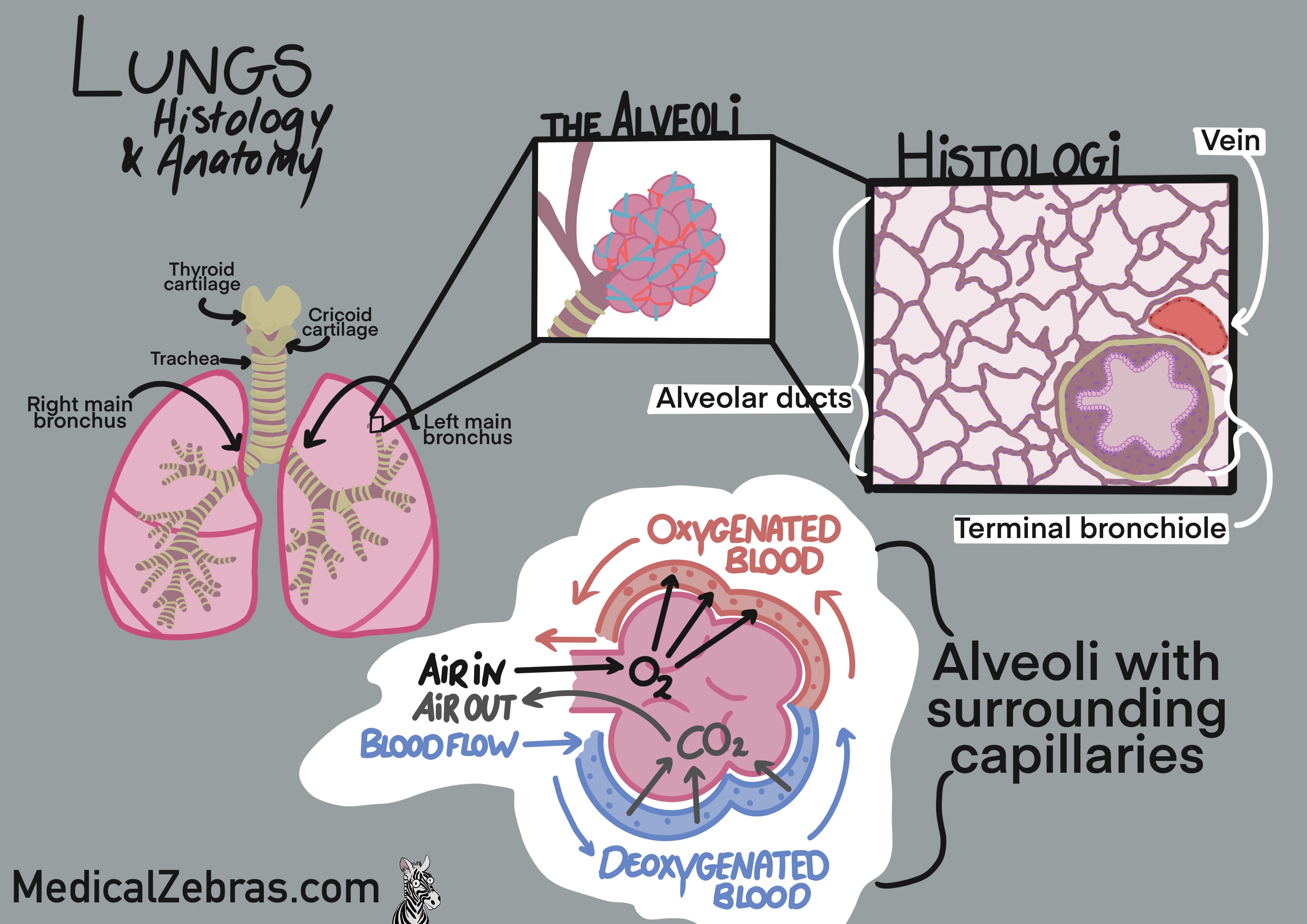
Histology
The histology of the lungs reveals a complex structure designed to facilitate efficient gas exchange. The lungs are primarily composed of alveoli, which are tiny, balloon-like structures lined with a single layer of squamous epithelial cells called type I pneumocytes. These cells are thin and flat, allowing for rapid diffusion of gases. Interspersed among the type I pneumocytes are type II pneumocytes, which are cuboidal cells responsible for producing surfactant, a substance that reduces surface tension and prevents alveolar collapse during exhalation. The alveoli are surrounded by a dense network of capillaries, where the exchange of oxygen and carbon dioxide occurs. The walls of the alveoli and capillaries are extremely thin, facilitating efficient gas exchange. The bronchi and bronchioles are lined with ciliated pseudostratified columnar epithelium, which contains goblet cells that produce mucus to trap foreign particles and pathogens. The cilia help move the mucus upward toward the throat for removal. The lungs also contain connective tissue, blood vessels, lymphatic vessels, and immune cells that contribute to their overall function and defense mechanisms.- Alveoli: lined with type I and type II pneumocytes
- Type I pneumocytes: thin squamous cells for gas exchange
- Type II pneumocytes: cuboidal cells producing surfactant
- Bronchi and bronchioles: lined with ciliated pseudostratified columnar epithelium
- Goblet cells: produce mucus to trap particles
- Capillaries: dense network surrounding alveoli for gas exchange
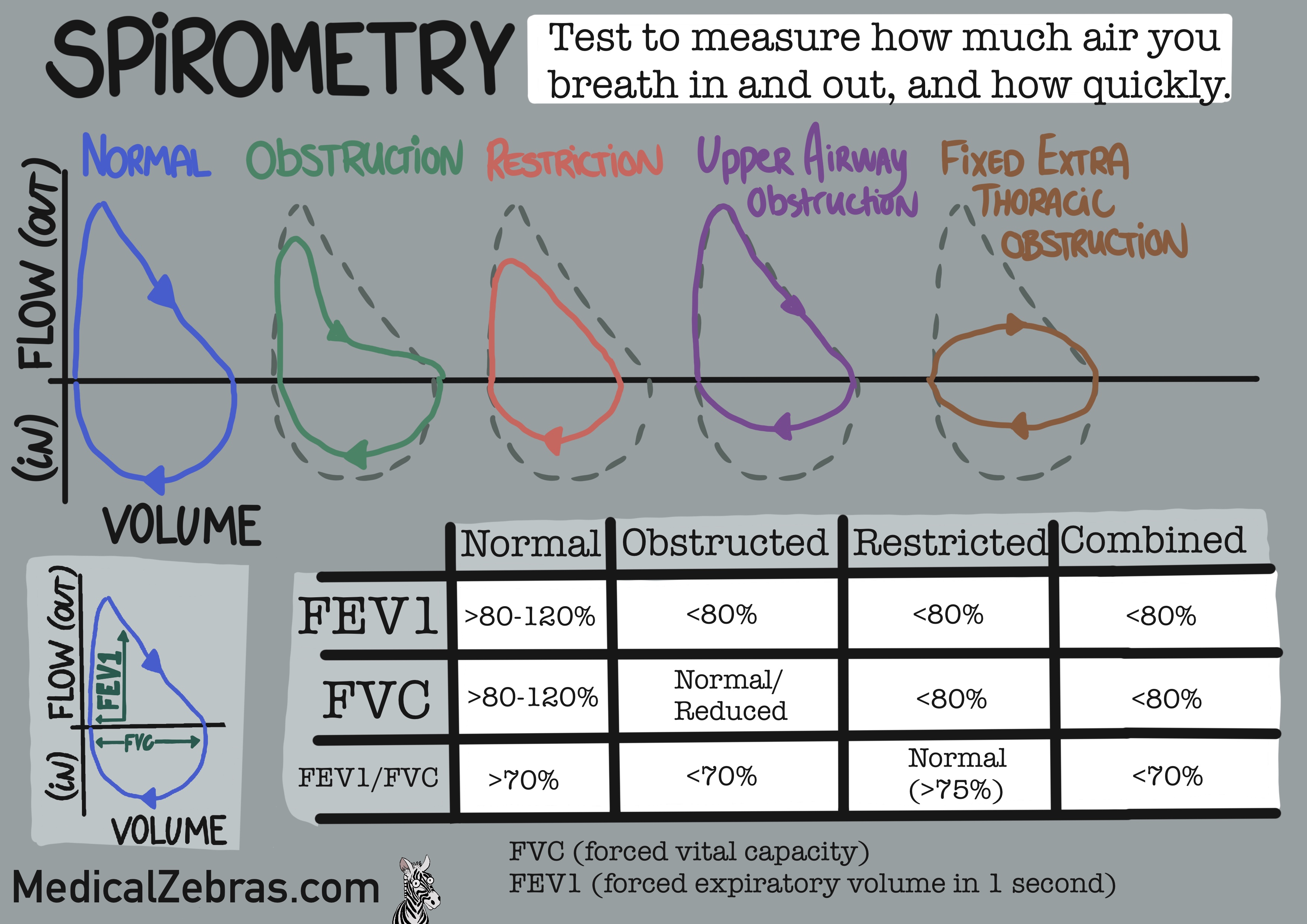
Spirometry
Spirometry is a common pulmonary function test that measures lung
function, specifically the volume and flow of air that can be inhaled
and exhaled. It is used to diagnose and monitor respiratory conditions
such as asthma, chronic obstructive pulmonary disease (COPD), and
other disorders that affect breathing. During a spirometry test, the
patient takes a deep breath and exhales forcefully into a device
called a spirometer. The spirometer records the amount of air exhaled
and the speed of the exhalation. Key measurements obtained from
spirometry include:
-
Forced Vital Capacity (FVC):
The total volume of air that can be forcefully exhaled after
taking a deep breath.
-
Forced Expiratory Volume in 1 second (FEV1):The volume of air that can be forcefully exhaled in the first
second of the FVC maneuver.
-
FEV1/FVC Ratio:
The ratio of FEV1 to FVC, expressed as a percentage. This ratio
helps to differentiate between obstructive and restrictive lung
diseases.
-
Peak Expiratory Flow (PEF):
The maximum speed of exhalation during the FVC maneuver.
-
Obstructive Lung Diseases:
reduced FEV1 and a decreased FEV1/FVC ratio, indicating airflow
obstruction. For example, asthma and COPD.
-
Restrictive Lung Diseases:
reduced FVC with a normal or increased FEV1/FVC ratio, indicating
restricted lung expansion. For example, pulmonary fibrosis and
sarcoidosis
Pathology
Astma
is a chronic inflammatory disease of the airways characterized by reversible airflow obstruction and bronchial hyperresponsiveness. It affects people of all ages and is often associated with allergies. The inflammation in asthma leads to swelling and narrowing of the airways, making it difficult to breathe. Common symptoms of asthma include wheezing, coughing, shortness of breath, and chest tightness. These symptoms can vary in severity and frequency, often triggered by factors such as allergens, respiratory infections, exercise, cold air, and stress. Asthma is typically diagnosed through a combination of clinical history, physical examination, and pulmonary function tests such as spirometry. Treatment for asthma usually involves the use of bronchodilators to relieve acute symptoms and inhaled corticosteroids to reduce airway inflammation. In addition, identifying and avoiding triggers is an important aspect of asthma management. With proper treatment and lifestyle adjustments, most individuals with asthma can lead normal, active lives.- Thickened basement membrane
- Mucus plugging of the airways
- Smooth muscle hypertrophy
- Goblet cell hyperplasia
- Eosinophilic infiltration
- Subepithelial fibrosis
- Mast cell infiltration
- Episodic wheezing (expiratory, noisy high-pitched sound, because of narrowed airways) and coughing, often worse at night or early morning.
- Shortness of breath and chest tightness.
- Reduced FEV1 and FEV1/FVC ratio on spirometry.
- Significant improvement in FEV1 after bronchodilator administration (reversibility).
- Peak expiratory flow variability (not often used)
- Elevated serum IgE and eosinophilia (in allergic asthma).
- Positive allergy testing (skin prick or specific IgE) only if the astma is allergic related.
- Inhaled corticosteroids
-
Bronchodilators (short-acting and long-acting)
- Short-acting beta-agonists (eg. albuterol and levalbuterol)
- Long-acting beta-agonists (eg. salmeterol and formoterol)
- Anticholinergics (eg. ipratropium and tiotropium)
- Leukotriene modifiers (eg. montelukast and zafirlukast)
- Allergen avoidance (eg. avoiding pollen, dust mites)
- Asthma action plan (personalized plan for managing symptoms and exacerbations)
-
Histology:
-
Symptoms:
-
Diagnosis:
-
Treatment:
Chronic Obstructive Pulmonary Disease (COPD)
is a progressive lung disease characterized by persistent airflow limitation that is not fully reversible. It is primarily caused by long-term exposure to noxious particles or gases, most commonly from cigarette smoking. COPD encompasses two main conditions: chronic bronchitis and emphysema. Chronic bronchitis is characterized by inflammation of the bronchial tubes, leading to increased mucus production and a chronic cough. Emphysema involves the destruction of the alveoli, resulting in reduced surface area for gas exchange and impaired oxygen uptake. Symptoms of COPD include chronic cough, sputum production, shortness of breath (especially during physical activity), and wheezing. As the disease progresses, individuals may experience frequent respiratory infections and exacerbations. Diagnosis of COPD is typically confirmed through spirometry, which shows a reduced FEV1/FVC ratio. Management of COPD involves smoking cessation, bronchodilator therapy, inhaled corticosteroids, pulmonary rehabilitation, and oxygen therapy in advanced cases. While COPD is a chronic condition, proper management can help improve quality of life and reduce symptoms.- Destruction of alveolar walls (emphysema)
- Enlarged airspaces
- Chronic inflammation of bronchi (chronic bronchitis)
- Mucus gland hyperplasia
- Goblet cell hyperplasia
- Smooth muscle hypertrophy
- Fibrosis of small airways
- Chronic cough with sputum production.
- Progressive shortness of breath, especially during physical activity.
- Wheezing and chest tightness.
- Frequent respiratory infections.
- Reduced FEV1 and FEV1/FVC ratio on spirometry.
- History of exposure to risk factors (eg. smoking, occupational hazards).
- Chest X-ray or CT scan showing hyperinflation and flattened diaphragm.
- Smoking cessation
-
Bronchodilators (short-acting and long-acting)
- Short-acting beta-agonists (eg. albuterol and levalbuterol)
- Long-acting beta-agonists (eg. salmeterol and formoterol)
- Anticholinergics (eg. ipratropium and tiotropium)
- Inhaled corticosteroids
- Pulmonary rehabilitation
- Oxygen therapy (in advanced cases)
-
Histology:
-
Symptoms:
-
Diagnosis:
-
Treatment:
Pulmonary Fibrosis
is a chronic and progressive lung disease characterized by the formation of scar tissue (fibrosis) in the lung interstitium, leading to impaired gas exchange and reduced lung function. The exact cause of pulmonary fibrosis is often unknown (idiopathic), but it can also result from exposure to environmental toxins, certain medications, radiation therapy, and underlying medical conditions such as autoimmune diseases. The fibrosis leads to thickening and stiffening of the lung tissue, making it difficult for the lungs to expand and contract during breathing. Symptoms of pulmonary fibrosis include progressive shortness of breath, a dry cough, fatigue, and unexplained weight loss. As the disease advances, individuals may experience clubbing of the fingers and cyanosis. Diagnosis is typically made through a combination of clinical history, pulmonary function tests, high-resolution CT scans, and sometimes lung biopsy. There is no cure for pulmonary fibrosis, but treatment options such as antifibrotic medications, oxygen therapy, and pulmonary rehabilitation can help manage symptoms and improve quality of life. In severe cases, lung transplantation may be considered.- Thickened alveolar walls
- Excessive collagen deposition
- Fibroblast proliferation
- Destruction of normal lung architecture
- Honeycomb lung appearance
- Chronic inflammation
- Progressive shortness of breath.
- Dry cough.
- Fatigue and unexplained weight loss.
- Clubbing of fingers (in advanced cases).
- FEV1 and FVC are reduced, with a normal or increased FEV1/FVC ratio.
- Reduced lung volumes (TLC, RV) on pulmonary function tests.
- High-resolution CT scan showing reticular opacities and honeycombing.
- Lung biopsy (in some cases) showing fibrosis and architectural distortion.
- Antifibrotic medications (eg. pirfenidone and nintedanib) that can slow disease progression by inhibiting fibroblast activity, reducing collagen production, and decreasing inflammation in the lungs.
- Oxygen therapy
- Pulmonary rehabilitation
- Lung transplantation (in severe cases)
-
Histology:
-
Symptoms:
-
Diagnosis:
-
Treatment:
Acute Respiratory Distress Syndrome (ARDS)
is a severe and life-threatening condition characterized by rapid onset of widespread inflammation in the lungs, leading to respiratory failure. It is often triggered by an underlying condition such as pneumonia, sepsis, trauma, or aspiration of gastric contents. In ARDS, the alveoli become damaged and filled with fluid, impairing gas exchange and leading to low oxygen levels in the blood (hypoxemia). Symptoms of ARDS include severe shortness of breath, rapid breathing, and cyanosis. The condition typically develops within hours to days after the initial insult. Diagnosis is based on clinical criteria, including the presence of bilateral infiltrates on chest imaging, hypoxemia, and the absence of cardiac failure as the primary cause. Treatment of ARDS involves supportive care in an intensive care unit, including mechanical ventilation to maintain adequate oxygenation, fluid management, and addressing the underlying cause. Despite advances in care, ARDS has a high mortality rate, and survivors may experience long-term respiratory complications.- Diffuse alveolar damage
- Hyaline membrane formation (pink/eosinophilic)
- Interstitial and alveolar edema
- Inflammatory cell infiltration
- Type II pneumocyte hyperplasia
- Fibrosis (in later stages)
- Severe shortness of breath.
- Rapid breathing.
- Cyanosis (bluish discoloration of the skin and mucous membranes).
- Bilateral infiltrates on chest X-ray or CT scan.
- Hypoxemia with a PaO2/FiO2 ratio ≤ 300 mmHg.
- Onset within one week of a known clinical insult or new/worsening respiratory symptoms.
- Absence of cardiac failure as the primary cause of respiratory failure.
- Mechanical ventilation with low tidal volumes
- Prone positioning
- Fluid management
- Treatment of underlying cause (eg. antibiotics for infection)
-
Histology:
-
Symptoms:
-
Diagnosis:
-
Treatment:
Pneumonia
is an infection that inflames the air sacs in one or both lungs, which may fill with fluid or pus. It can be caused by various pathogens, including bacteria, viruses, and fungi. Pneumonia can range from mild to severe and can affect people of all ages, although it is particularly dangerous for young children, the elderly, and individuals with weakened immune systems. Common symptoms of pneumonia include cough (with phlegm or pus), fever, chills, shortness of breath, chest pain, and fatigue. The infection can be acquired in the community (community-acquired pneumonia) or in healthcare settings (hospital-acquired pneumonia). Diagnosis is typically made through clinical evaluation, chest X-rays, and sputum cultures. Treatment depends on the underlying cause but often includes antibiotics for bacterial pneumonia, antiviral medications for viral pneumonia, and antifungal drugs for fungal pneumonia. Supportive care, such as rest, fluids, and oxygen therapy, may also be necessary. With prompt and appropriate treatment, most individuals recover fully from pneumonia, although severe cases can lead to complications such as respiratory failure or sepsis.-
Common
bacteria
causing pneumonia:
- Streptococcus pneumoniae (most common cause of community-acquired pneumonia)
- Haemophilus influenzae (common cause of bacterial pneumonia) - PCR of respiratory secretions
- Mycoplasma pneumoniae (atypical pneumonia) - PCR of respiratory secretions
- Chlamydophila pneumoniae (atypical pneumonia)
- Legionella pneumophila (atypical pneumonia, associated with contaminated water sources) - antigen detection in urine or PCR of respiratory secretions
- Klebsiella pneumoniae (common cause of hospital-acquired pneumonia) - a "currant jelly" sputum appearance - PCR of respiratory secretions
- Staphylococcus aureus (common cause of hospital-acquired pneumonia)
-
Common
viruses
causing pneumonia:
- Influenza virus (common in all age groups)
- Respiratory syncytial virus (RSV) (common in infants and young children)
- Coronavirus (including SARS-CoV-2) (common in all age groups)
- Adenovirus (common in children)
- Parainfluenza virus (common in children)
-
Common
fungi
causing pneumonia:
- Histoplasma capsulatum ( common in certain geographic areas, such as the Ohio and Mississippi River valleys)
- Coccidioides immitis (common in certain geographic areas, such as the southwestern United States)
- Cryptococcus neoformans (common in immunocompromised patients; eg. those with HIV/AIDS or on immunosuppressive therapy)
- Pneumocystis jirovecii (common in immunocompromised patients; eg. those with HIV/AIDS or on immunosuppressive therapy)
- Alveolar inflammation
- Exudate in alveolar spaces
- Neutrophil infiltration
- Congested capillaries
- Fibrin deposition
- Type II pneumocyte hyperplasia
- Cough with phlegm or pus.
- Fever and chills.
- Shortness of breath.
- Chest pain.
- Fatigue. Atypical symptoms (more common in atypical pneumonia):
- Dry cough.
- Low-grade fever.
- Headache.
- Muscle aches.
- Elevated white blood cell count.
- Stethoscope examination revealing abnormal lung sounds, such as crackles or ronchi, and dullness on percussion.
- Chest X-ray showing infiltrates, consolidation, or other abnormalities.
- Sputum culture identifying the causative pathogen, however, if atypical pneumonia is suspected, PCR of respiratory secretions is preferred as it would otherwise be difficult to identify the pathogen.
- Antibiotics (for bacterial pneumonia)
- Antiviral medications (for viral pneumonia)
- Antifungal drugs (for fungal pneumonia)
- Supportive care (rest, fluids, oxygen therapy)
-
Histology:
-
Symptoms:
-
Diagnosis:
-
Treatment: