Anatomy
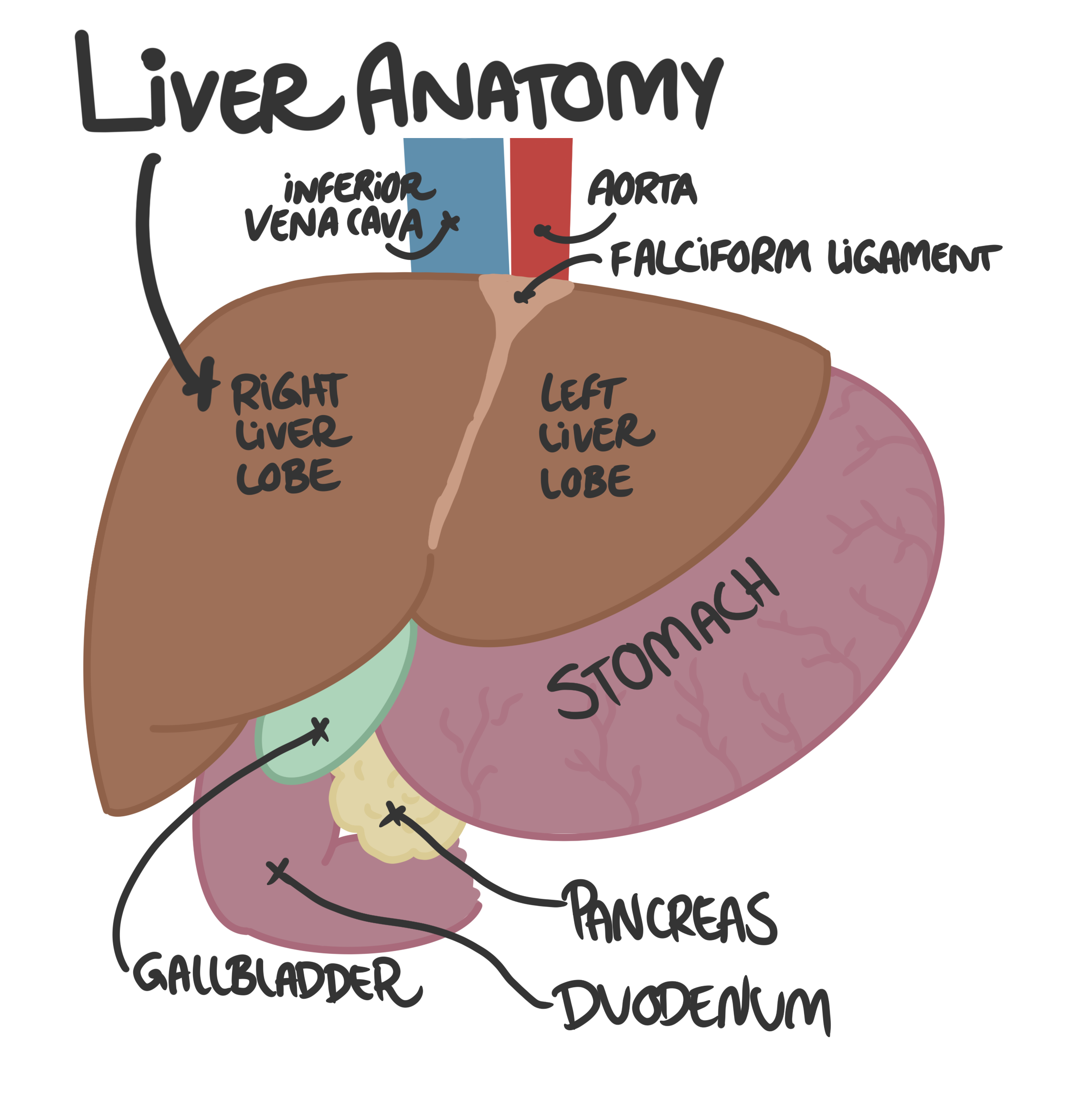
The liver is the largest internal organ in the body and has many functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion. The liver is divided into four lobes: right, left, caudate, and quadrate. The liver receives blood from two main sources:- the hepatic artery, which supplies oxygenated blood, and
- the portal vein, which brings nutrient-rich blood from the gastrointestinal tract.
The liver is surrounded by a connective tissue capsule called Glisson's capsule.
Histology
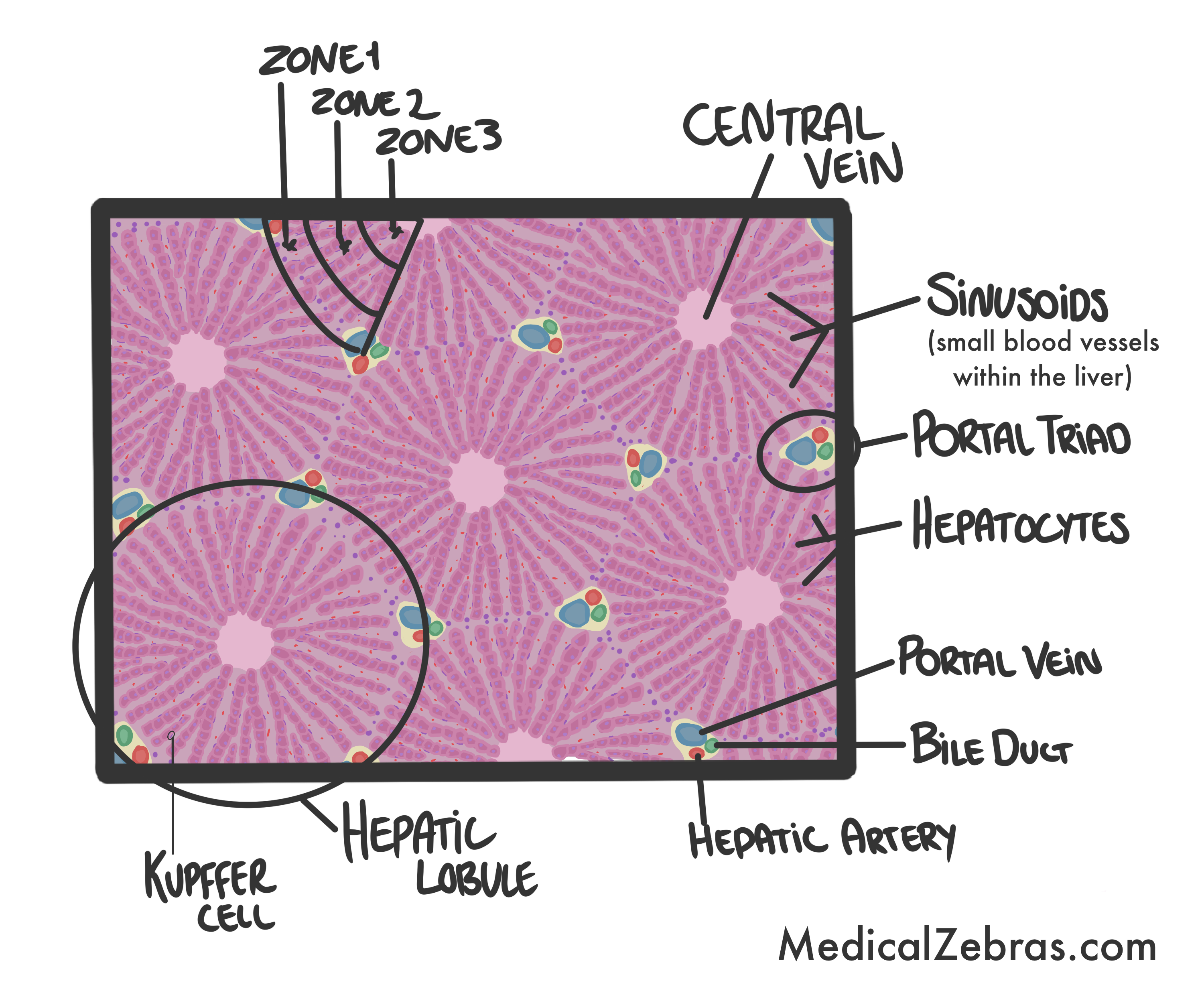
- Hepatic lobules: The functional units of the liver, consisting of hepatocytes arranged in plates around a central vein.
- Portal triads: Located at the corners of the hepatic lobules, containing a branch of the hepatic artery, a branch of the portal vein, and a bile duct.
- Sinusoids: Specialized capillaries that allow blood to percolate through the liver.
- Kupffer cells: Specialized macrophages located in the sinusoids that help to remove debris and pathogens from the blood.
-
Zone 1 (periportal zone):
Closest to the portal triad, receives the most oxygenated blood,
and is the first to be affected by toxins.
-
Zone 2 (intermediate zone):
Intermediate zone between zones 1 and 3. Here the hepatocytes
perform various metabolic functions.
-
Zone 3 (centrilobular zone):
Closest to the central vein, receives the least oxygenated
blood, and is most susceptible to ischemic injury.
Pathology
Hepatitis
Is an inflammation of the liver that can be caused by viral infections (such as hepatitis A, B, C, D, and E), alcohol abuse, toxins, or autoimmune diseases. In hepatitis, you will see hepatocyte necrosis, inflammatory infiltrates (mainly lymphocytes and macrophages) in the portal tracts and lobules, and ballooning degeneration of hepatocytes. In chronic hepatitis, you may also see fibrosis and cirrhosis.- Fatigue
- Jaundice (often first evident in the sclera of the eyes)
- Abdominal pain (often in the right upper quadrant)
- Nausea and vomiting
- Elevated liver enzymes (ALT, AST)
- may be asymptomatic for years but can eventually lead to cirrhosis and liver failure.
- IgM anti-HAV for hepatitis A
- HBcAg for hepatitis B, a core antigen indicating active infection that appears during acute or chronic infection.
- anti-HCV for hepatitis C, a marker of exposure to the virus and indicates current or past infection.
- Acute hepatitis: usually supportive care, including rest, hydration, and avoiding alcohol and hepatotoxic drugs. Most cases resolve spontaneously. However, specific antiviral therapy may be required for hepatitis B and C infections.
- Chronic hepatitis: may require antiviral therapy for hepatitis B and C to reduce viral load and prevent progression to cirrhosis. In severe cases corticosteroids or immunosuppressive drugs may be used for autoimmune hepatitis. Lifestyle modifications such as avoiding alcohol and maintaining a healthy weight are also important.
-
Symptoms:
-
Acute hepatitis:
Chronic hepatitis:
-
Diagnosis:
-
Acute hepatitis:
-
Blood tests showing elevated liver enzymes (ALT, AST)
-
Serological tests for viral hepatitis markers, such as
-
HBsAg for hepatitis B, indicating chronic infection if
present for more than six months.
-
anti-HCV for hepatitis C, indicating chronic infection if
RNA is detected in the blood.
-
Liver biopsy may be performed to assess the degree of
inflammation and fibrosis.
-
imaging studies such as ultrasound or elastography to
assess liver stiffness and fibrosis.
-
Treatment:
Fatty liver disease (steatosis)
Is characterized by the accumulation of fat within hepatocytes. This can be caused by alcohol abuse (alcoholic fatty liver disease) or metabolic conditions such as obesity, diabetes, and hyperlipidemia (non-alcoholic fatty liver disease). In fatty liver disease, you will see macrovesicular steatosis, where large fat droplets displace the nucleus to the periphery of the hepatocyte.-
Non-alcoholic fatty liver disease (NAFLD):
often asymptomatic but can sometimes cause fatigue,
hepatomegaly, and elevated liver enzymes.
-
Overweight/obesity, diabetes, hyperlipidemia, and
metabolic syndrome are common risk factors for
NAFLD.
- Alcoholic fatty liver disease: often asymptomatic but can sometimes cause fatigue, hepatomegaly, elevated liver enzymes, and signs of alcohol abuse.
- Non-alcoholic fatty liver disease (NAFLD): is typically made through imaging studies (ultrasound, CT scan) that show increased liver echogenicity, and can be confirmed with a liver biopsy.
- Alcoholic fatty liver disease: is typically made through a combination of clinical presentation, laboratory tests (elevated liver enzymes, elevated mean corpuscular volume (MCV), and carbohydrate-deficient transferrin (CDT)), and imaging studies (ultrasound, CT scan) that show increased liver echogenicity, and can be confirmed with a liver biopsy.
- Non-alcoholic fatty liver disease (NAFLD): usually involves lifestyle changes such as weight loss, dietary modifications, and management of underlying conditions like diabetes and hyperlipidemia.
- Alcoholic fatty liver disease: abstaining from alcohol is crucial.
-
Symptoms:
-
Diagnosis:
-
Treatment:
Alcoholic hepatitis
Is an acute inflammation of the liver caused by excessive alcohol consumption. In alcoholic hepatitis, histologically you will see hepatocyte ballooning, neutrophilic infiltrates, Mallory-Denk bodies (cytoplasmic inclusions composed of damaged intermediate filaments), and pericellular fibrosis.- Jaundice
- Fever
- Right upper quadrant abdominal pain
- Nausea and vomiting
- Hepatomegaly
- Blood tests showing elevated liver enzymes (ALT, AST) with an AST/ALT ratio >2, elevated bilirubin, and prolonged prothrombin time.
- Imaging studies such as ultrasound or CT scan may show an enlarged liver with a heterogeneous echotexture.
- Liver biopsy may be performed to confirm the diagnosis and assess the severity of liver damage.
- Abstinence from alcohol is crucial.
- Supportive care, including nutritional support and management of complications such as infections and encephalopathy.
- In severe cases, corticosteroids or pentoxifylline may be used to reduce inflammation.
-
Symptoms:
-
Diagnosis:
-
Treatment:
Cirrhosis
Is the end-stage of chronic liver disease characterized by
fibrosis and the formation of regenerative nodules. It can
result from various causes, including chronic hepatitis, alcohol
abuse, and non-alcoholic fatty liver disease. In cirrhosis, you
will see
extensive fibrosis that disrupts the normal liver
architecture, regenerative nodules of hepatocytes, and
portal hypertension.
- Early stages may be asymptomatic or present with fatigue and mild hepatomegaly.
- Advanced stages may present with signs of liver failure and portal hypertension, such as jaundice, ascites, variceal bleeding (especially esophageal varices, this is due to increased pressure in the portal vein causing blood to be diverted to smaller veins that can rupture) , hepatic encephalopathy (confusion, asterixis, and altered level of consciousness, caused by accumulation of toxins like ammonia in the brain ), and spider angiomas (sign of high estrogen).
- treating the underlying cause (such as antiviral therapy for hepatitis or abstinence from alcohol).
-
managing complications of cirrhosis
-
Ascites (with diuretics and paracentesis (removal of
fluid from the abdomen by a needle inse rtion into the
peritoneal cavity and draining the fluid out))
-
Variceal bleeding (with endoscopic band ligation or
sclerotherapy)
-
Hepatic encephalopathy (with lactulose and rifaximin)
- in severe cases, liver transplantation may be necessary.
-
Symptoms:
-
Diagnosis:
-
Blood test:
-
Bilirubin (elevated in liver dysfunction)
-
Albumin (decreased in liver dysfunction)
-
Prothrombin time (prolonged in liver dysfunction, as the
liver fails to produce clotting factors)
-
Platelet count (decreased in portal hypertension,
because of splenic sequestration which is enlarged due
to portal hypertension and causes thrombocytopenia ,
leukopenia and anemia as blood cells are being
sequestered in the enlarged spleen )
-
Ultrasound, CT scan, or MRI may show a nodular liver
surface, splenomegaly, and signs of portal hypertension
(such as dilated portal vein and collateral vessels).
-
may be performed to confirm the diagnosis and assess the
degree of fibrosis. The biopsy will show extensive
fibrosis and regenerative nodules.
-
Treatment:

Liver cancer (hepatocellular carcinoma)
Is a primary malignancy of the liver that often arises in the setting of chronic liver disease and cirrhosis.Histology: malignant hepatocytes form trabecular, pseudoglandular, or solid patterns, with cellular atypia and increased mitotic activity. You may also see vascular invasion and necrosis. The cells may sometimes produce alpha-fetoprotein (AFP), which can be used as a tumor marker, and used to monitor treatment response and disease recurrence. Other features include fibrous septa and bile production by the tumor cells, which can be seen as bile plugs within the tumor.
Genetics: common genetic alterations in liver cancer include mutations in the TP53 tumor suppressor gene, activation of the Wnt/β-catenin signaling pathway, and amplification of the MYC oncogene.
- Weight loss
- Abdominal pain
- Hepatomegaly
- Jaundice
- sometimes elevated alpha-fetoprotein (AFP) levels
- Elevated alpha-fetoprotein (AFP) levels in the blood, although not all cases of liver cancer will have elevated AFP.
- Imaging studies such as ultrasound, CT scan, or MRI may show a liver mass with characteristic features of liver cancer, such as arterial enhancement and washout in the venous phase.
- Liver biopsy
- Surgical resection may be an option for patients with early-stage liver cancer and good liver function.
- Liver transplantation may be considered for patients with small tumors and underlying cirrhosis.
- Locoregional therapies such as radiofrequency ablation (RFA) or transarterial chemoembolization (TACE) may be used for patients with intermediate-stage liver cancer.
- Systemic therapies such as targeted therapy (e.g., sorafenib) or immunotherapy (e.g., nivolumab) may be used for patients with advanced-stage liver cancer.
-
Symptoms:
-
Diagnosis:
-
Treatment:
Depends on various factors, including the stage of the cancer, liver function, and overall health of the patient.
Liver abscess
Is a localized collection of pus within the liver parenchyma, usually caused by bacterial, fungal, or parasitic infections. In liver abscess, you will see necrotic tissue, pus, and inflammatory infiltrates (mainly neutrophils) within the abscess cavity.- fever & chills
- Right upper quadrant pain, the pain can in some cases radiate to the shoulder or chest
- Jaundice
- Hepatomegaly
- Elevated white blood cell count (indicating infection) and liver enzymes (ALT, AST) (indicating liver inflammation).
- ultrasound or CT scan may show a hypoechoic or hypodense lesion with irregular borders and surrounding edema.
- Aspiration of the abscess under imaging guidance for microbiological analysis and culture to identify the causative organism.
- Antibiotics: broad-spectrum antibiotics are usually started empirically and then tailored based on culture results.
- Drainage: percutaneous drainage under imaging guidance is often preferred for larger abscesses or those that do not respond to antibiotics alone. Surgical drainage may be necessary in some cases, especially if there are multiple abscesses or if the abscess is located in a difficult-to-access area (such as near major blood vessels).
-
Symptoms:
-
Diagnosis:
-
Blood tests:
-
Treatment:
Hemochromatosis
Is a genetic disorder characterized by excessive absorption and accumulation of iron in the body, leading to iron overload in various organs, such as the skin, pancreas, heart, and liver.Genetics: mutations in the HFE gene, which is involved in the regulation of iron absorption from the diet. The most common mutations are C282Y and H63D. It is inherited in an autosomal recessive manner.
Histology: iron deposits within hepatocytes and
Kupffer cells, which can be visualized using special stains such
as Prussian blue. As the disease progresses, it can lead to
hepatocyte necrosis, inflammatory infiltrates, and
fibrosis. The symptoms often present in middle age, when iron
accumulation reaches toxic levels.
- Fatigue
- Joint pain (especially in the hands and feet)
- Abdominal pain, caused by liver enlargement
- Hepatomegaly can lead to cirrhosis and liver failure if untreated
- Skin hyperpigmentation (bronze or gray discoloration), patients may look tanned even without sun exposure
- Diabetes mellitus (due to iron deposition in the pancreas, that lead to damage)
- Cardiomyopathy (due to iron deposition in the heart, leading to heart failure and arrhythmias)
- Hypogonadism (due to iron deposition in the pituitary gland, leading to decreased production of sex hormones), which can cause infertility and loss of libido
- Women are often diagnosed later than men because they lose iron through menstruation and pregnancy, which can delay the onset of symptoms.
- Elevated serum ferritin and transferrin saturation levels, which indicate increased iron stores in the body.
- Genetic testing for HFE mutations (C282Y and H63D) to confirm the diagnosis.
- > If necessary, liver biopsy may be performed to assess the degree of iron deposition and liver damage.
- Phlebotomy (regular blood removal) is the mainstay of treatment to reduce iron levels in the body.
- Dietary modifications to limit iron intake, such as avoiding iron supplements and reducing consumption of red meat and alcohol.
-
Symptoms:
-
Diagnosis:
-
Treatment:
Wilson's disease
Is a genetic disorder characterized by impaired copper metabolism, leading to copper accumulation in various organs, including the liver. In Wilson's disease, you will see copper deposits within hepatocytes, which can be visualized using special stains such as rhodanine or orcein. The genetic defect is in the ATP7B gene, which encodes a copper-transporting ATPase, and leads to decreased biliary copper excretion and increased copper accumulation. It is inherited in an autosomal recessive manner.As the disease progresses, it can lead to hepatocyte necrosis, inflammatory infiltrates, and fibrosis. The symptoms often present in adolescence or early adulthood, when copper accumulation reaches toxic levels. The copper accumulates primarily in the liver, causing liver damage and dysfunction, but also in other organs such as the brain, kidneys, and eyes. In the brain the copper accumulates mainly in the basal ganglia, and may lead to movement disorders such as tremors, dystonia, and parkinsonism, as well as psychiatric symptoms such as depression, anxiety, and psychosis, and with time cognitive decline. In the eyes, copper accumulation can lead to the formation of Kayser-Fleischer rings, which are brownish or greenish rings around the cornea (sign of long standing accumulation). In the kidneys, copper accumulation can lead to renal tubular dysfunction and Fanconi syndrome (leading to loss of glucose, amino acids, phosphate, and bicarbonate in the urine).
- Liver symptoms: fatigue, jaundice, abdominal pain, hepatomegaly, and signs of liver failure (ascites, variceal bleeding, hepatic encephalopathy).
- Neurological symptoms: tremors, dystonia, parkinsonism, dysarthria, and ataxia.
- Psychiatric symptoms: personality changes, mood disorders, and psychosis.
- Other symptoms: hemolytic anemia, renal tubular dysfunction, and Kayser-Fleischer rings (copper deposits / brown stain around the outer side of the cornea, only seen if the disease goes untreated for many years).
- Low serum ceruloplasmin levels (a copper-binding protein that is typically low in Wilson's disease).
- Elevated 24-hour urinary copper excretion (indicating increased copper accumulation in the body).
- Genetic testing for ATP7B mutations to confirm the diagnosis.
- Liver biopsy with quantitative copper analysis may be performed to assess the degree of copper accumulation in the liver.
- Pemphigus agents: such as penicillamine or trientine to promote copper excretion.
- Zinc therapy: to inhibit copper absorption from the gastrointestinal tract.
- Dietary modifications: to limit copper intake, such as avoiding foods high in copper (liver, shellfish, nuts, chocolate, and mushrooms).
- Liver transplantation: may be necessary in cases of severe liver damage or failure.
-
Symptoms:
-
Diagnosis:
-
Treatment: