Anatomy & Histology & Function
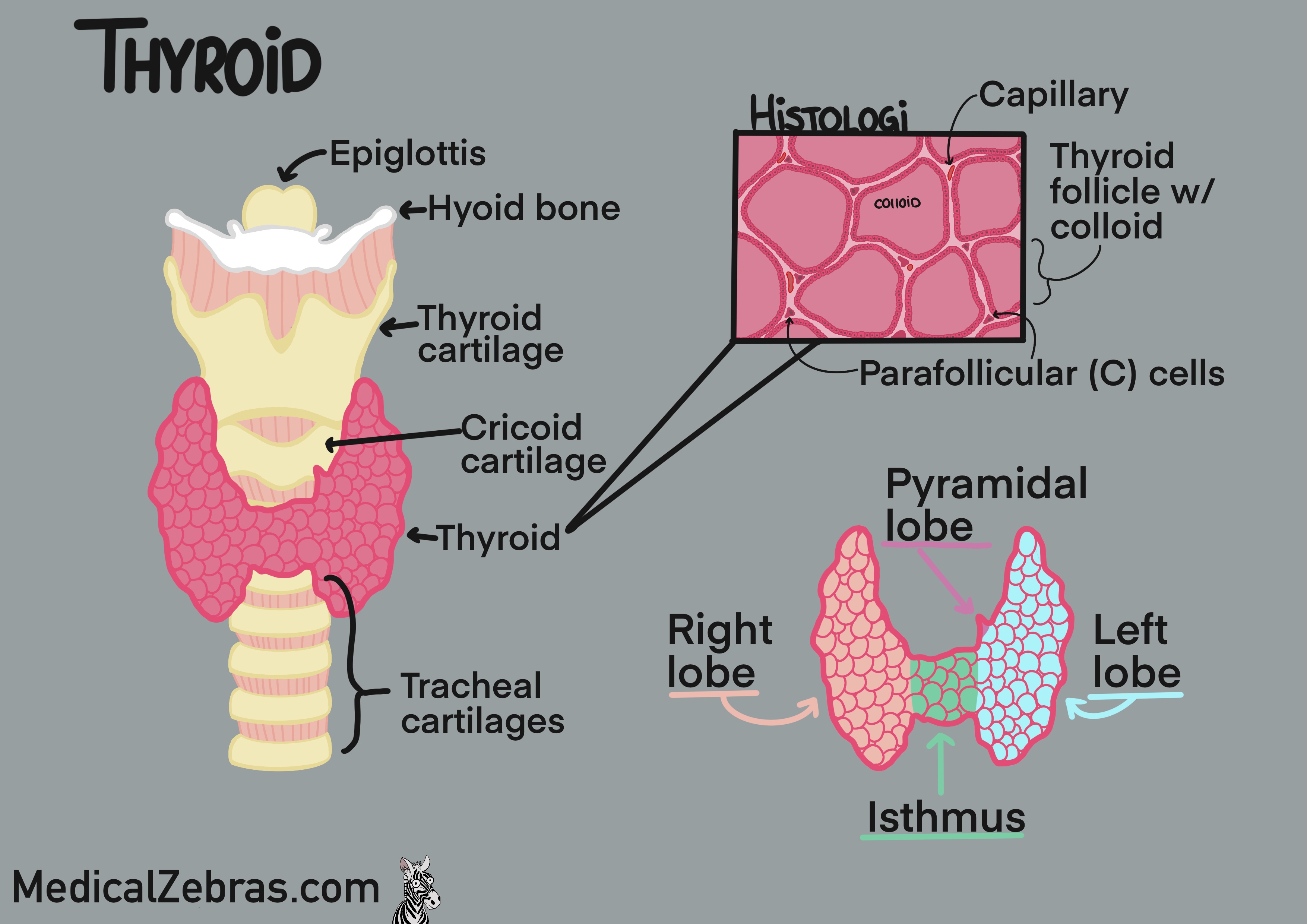
The thyroid gland is a butterfly-shaped gland located in the front of
the neck, just below the larynx. It consists of two lobes, one
on each side of the trachea, connected by a thin piece of tissue
called the isthmus. As the thyroid gland is formed it moves
from the base of the tongue to its final position in the neck via the
thyroglossal duct. Because of this migration, the thyroid gland can
sometimes be found in other locations, such as higher up in the neck
or even in the chest, known as an ectopic thyroid gland. Most often
you end up with a small strip of thyroid gland extending superiorily
from the isthmus, also called the pyramidal lobe.
Histologically the thyroid gland is made up of spherical structures called follicles, which are lined with a single layer of epithelial cells called follicular cells. The follicles are filled with a substance called colloid, which contains the precursor to thyroid hormones. (T3 and T4). Surrounding the follicles are parafollicular cells (also known as C-cells), which produce the hormone calcitonin. Between the follicles are connective tissue and blood vessels allowing for efficient transport of hormones.
Histology:
Histologically the thyroid gland is made up of spherical structures called follicles, which are lined with a single layer of epithelial cells called follicular cells. The follicles are filled with a substance called colloid, which contains the precursor to thyroid hormones. (T3 and T4). Surrounding the follicles are parafollicular cells (also known as C-cells), which produce the hormone calcitonin. Between the follicles are connective tissue and blood vessels allowing for efficient transport of hormones.
Histology:
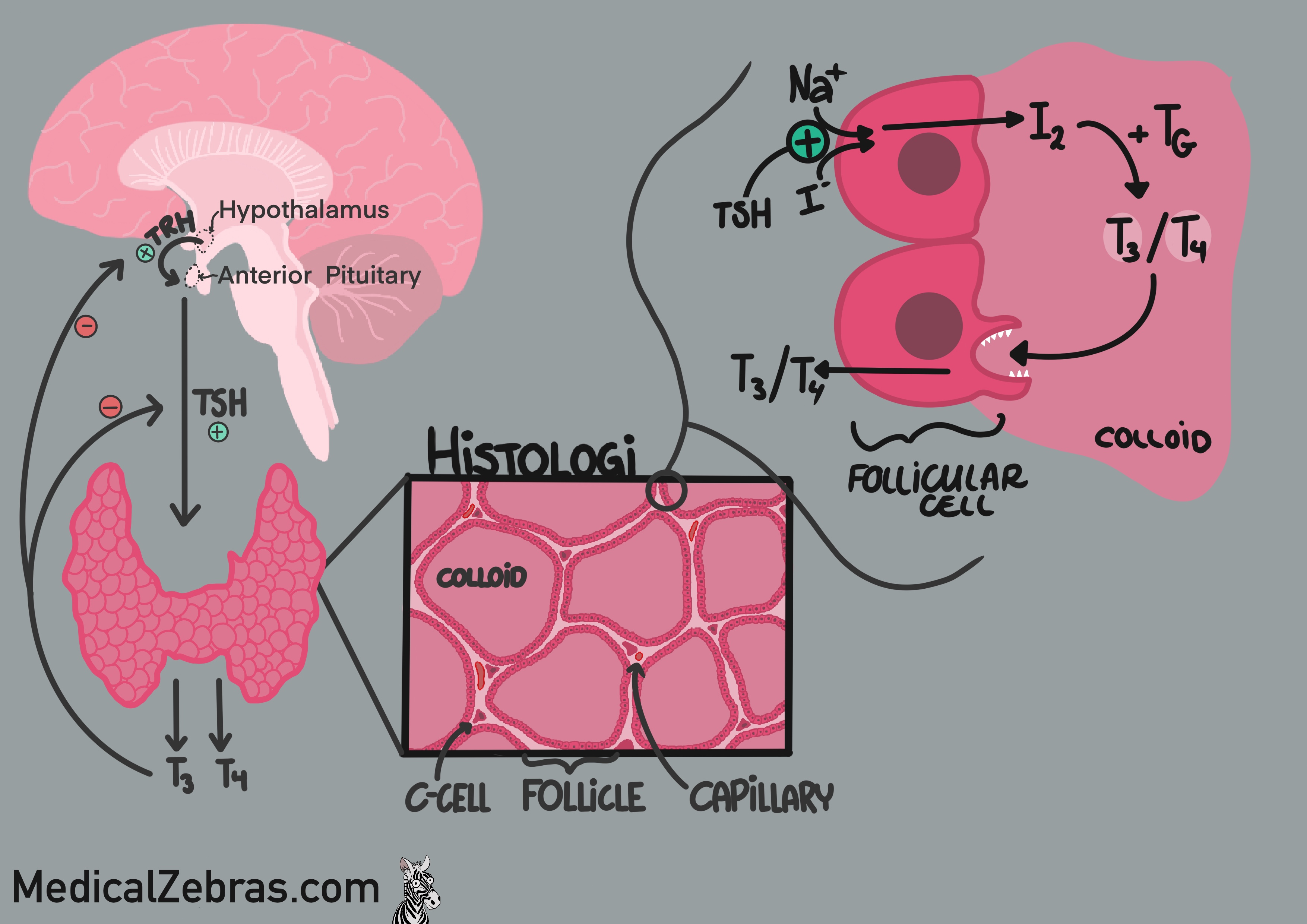
- Follicular cells (epithelial cells) take up iodine and release it into the colloid where it is used to make precursers of T3 and T4. Which is then taken up by the follicular cells, again, cleaved by proteases, and released into the blood stream as T3 and T4.
- Colloid contains thyroglobulin, a protein that is used to make thyroid hormones.
- Parafollicular cells (C-cells) produce the hormone calcitonin, which inhibits osteoclast activity (cells that break down bone and release calcium into the blood), and also promote the excretion of calcium and phosphate in the kidneys. This results in a decrease in blood calcium levels.
How to activate the thyroid gland: The journey start in the
hypothalamus where the thyroid receptor hormone (TRH) is
secreted. This hormone than stimulates the anterior pituitary gland to
secrete thyroid stimulating hormone (TSH). TSH travels to the
thyroid where it connects to a transporter on the outer side of the
follicular cells, which then activates a channel called the
sodium-iodide symporter (NIS). This channel then takes up iodine and
along with natrium transports it from the blood into the follicular
cell. The iodine is oxidized within the cell and transferred into the
lumen of the follicle or the colloid. Here the iodine is combined to
tyrosine inside a protein called thyroidglobulin, becoming MIP and
DIP. MIP and DIP are then combined to form T3 and T4, which are still
bound to the thyroglobulin. When the body needs thyroid hormones, the
follicular cells endocytose ("eat") some of the colloid containing the
thyroglobulin with T3 and T4 attached. The vesicle containing the
colloid fuses with a lysosome, where proteases cleave T3 and T4 from
the thyroglobulin. The free T3 and T4 are then released into the
bloodstream. In the blood, most of T3 and T4 are bound to carrier
proteins, such as thyroxine-binding globulin (TBG),
transthyretin, and albumin. Only a small fraction of T3 and T4 are
free and biologically active. T4 is converted to the more active T3 in
peripheral tissues by the enzyme deiodinase. T3 then enters cells and
binds to thyroid hormone receptors in the nucleus, where it regulates
gene expression and affects metabolism, growth, and development.
Diagnostic methods
Blood test
To test how the thyroids function, most often "TSH", "T3" and "T4" are checked.- Normal thyroid function Normal levels of T3, T4 and TSH.
- Hypoactive thyroid Low levels of T3 & T4, with high levels of TSH. Here the thyroid is not responding to TSH, so in response the anterior pituitary increase its release of TSH in hopes of normalising the low levels. If the T4 levels are normalised, it is called subclinical hypothyroidism.
-
Hyperactive thyroid High levels of T3 & T4, with low levels of
TSH. Here the thyroid is secreting too much of T3 & T4 causing
symptoms of a hyperactive thyroid gland. These high levels act as
negative stimulus on the anterior pituitary which then decreases its
TSH secreation. However, if TSH levels are also high, the problem does
not lie within the thyroid gland, but in a hyperactive anterior
pituitary, if TRH levels are normal or decreased, indicating a tumor
within the anterior pituitary. And if TRH levels are high, the
hypothalamus is the main problem, indicating that there might be a
tumor there.
If the levels of T3 and T4 are normalised, and TSH is low, it is called subclinical hyperthyroidism. - Thyroid antibody tests can be used to diagnose autoimmune thyroid disorders, such as Hashimoto's thyroiditis and Graves' disease. Common antibodies tested for include anti-thyroid peroxidase (anti-TPO) antibodies ( positive in Hashimoto's thyroiditis and Graves' disease ), TRAb (Thyroid-stimulating hormone receptor antibodies, positive in Graves' disease), and anti-thyroglobulin antibodies (positive in Hashimoto's thyroiditis).
Imaging
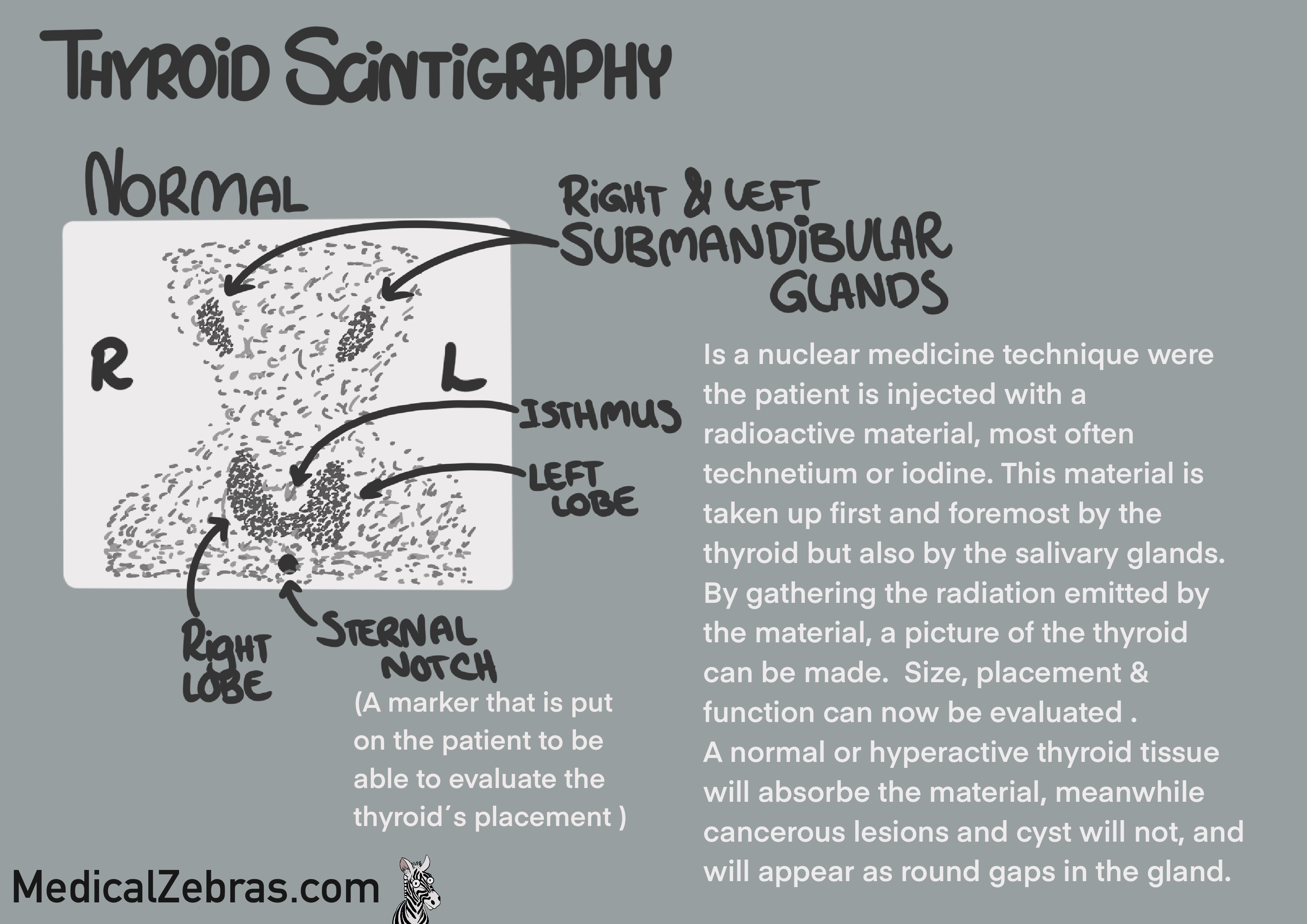
Thyroid Scintigraphy
Thyroid scintigraphy is a nuclear imaging technique that uses small amounts of radioactive material to evaluate the function and structure of the thyroid gland. The patient is injected with a small amount of radioactive iodine or technetium, which is taken up by the thyroid gland. A special camera, collimator, is used to detect and gather the radiation emitted by the radioactive material, and you are able to visualise the gland. As the radioactive material is also taken up by the salivary glands, most often they can be visualised as well.
Pros:
- Great way to easily assess the thyroid tissue function
- Cannot detect lesions under 1 cm.
- Cannot detect cold/hypofunctioning lesions if there is normal thyroid tissue in front or behind (here a SPECT/CT would be preferred, as you can then inspect the uptake in 3-D).
- Radioactive material is used.
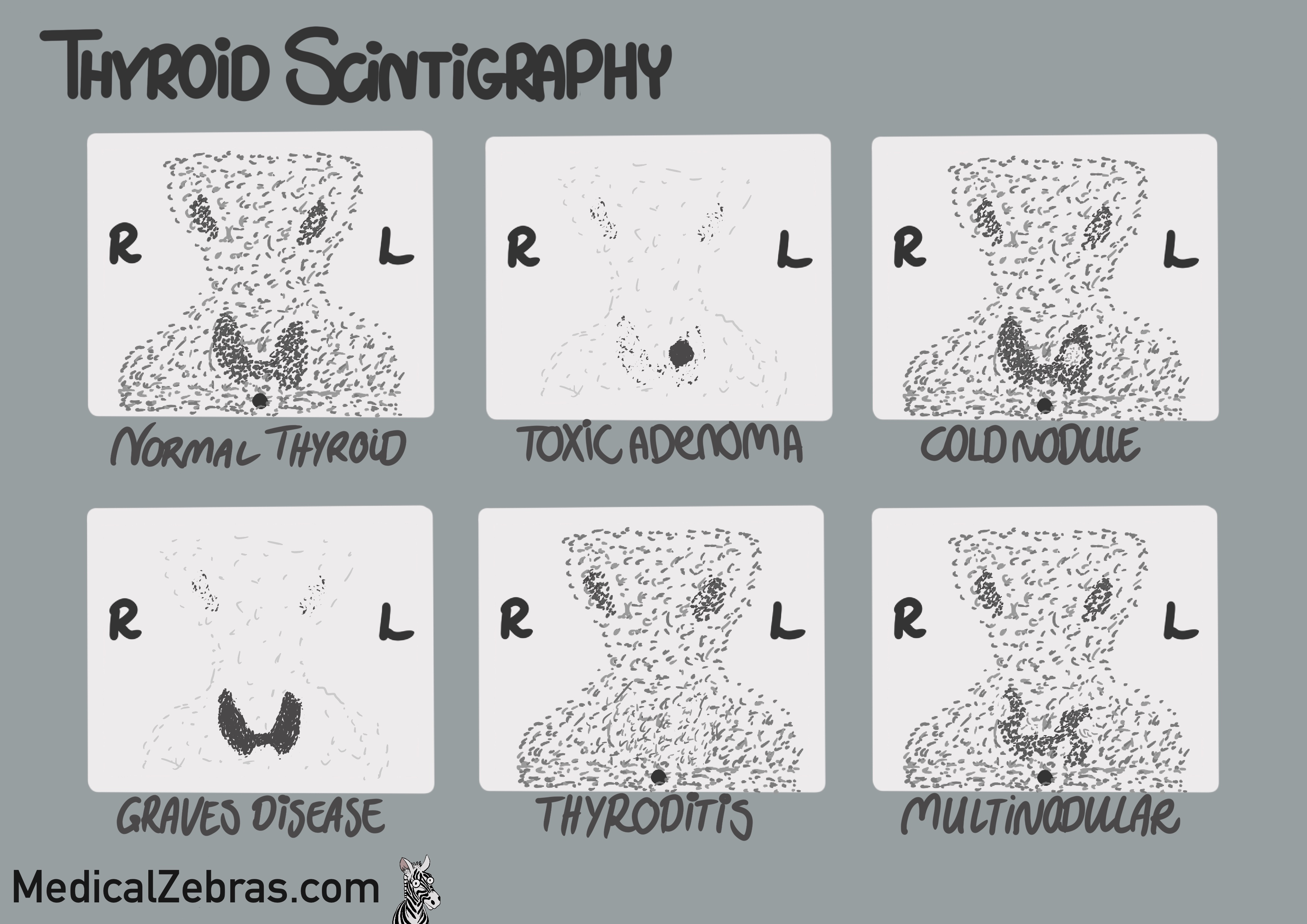
Interpretation
- Normal scan: Uniform uptake of the radioactive material throughout the thyroid gland, indicating normal function. You will also see uptake in the salivary glands.
- Hyperactive thyroid or nodule (hot/toxic nodule): Increased uptake of the radioactive material throughout the thyroid or in a specific area, indicating hyperfunctioning tissue. Simulatiously, there will be decreased uptake in the salivary glands and also the rest of the thyroid gland (if it is a nodule) as the hyperfunctioning tissue is taking up most of the radioactive material.
- Hypoactive thyroid nodule (cold nodule): Decreased uptake of the radioactive material in a specific area of the thyroid gland, indicating hypofunctioning tissue. As there is a small risk of a hypoactive nodule being malignant, further investigation with ultrasound is needed to evaluate the structure of the nodule, to further evaluate the risk of malignancy and the need for a biopsy. But this can also be due to benign causes such as cysts or colloid nodules.
- Multinodular goiter: Multiple areas of increased and decreased uptake of the radioactive material throughout the thyroid gland, indicating the presence of multiple nodules with varying levels of function.
- Diffuse decreased uptake of the radioactive material throughout the thyroid gland, and normal uptake in the salivary glands. Could indicate inflammation (thyroiditis) or be caused by iodine-induced hypothyroidism, or the presence of medications that interfere with iodine uptake (such as amiodarone or lithium, or levothyroxine (decreases TSH)) or iodine-containing contrast agents (used for CT-scans) that compete for thyroid uptake.
-
Artifacts:
- Uptake in the esophagus or stomach if the patient has swallowed some of the radioactive material, that has been secreted into the saliva and then swallowed. Drinking water before the scan can help reduce this artifact.
- High levels of circulating thyroid hormones, which can suppress the uptake of the radioactive material. This can be seen in patients with hyperthyroidism or thyroiditis.
Ultrasound
Ultrasound is most often used to evaluate the size and shape of the
thyroid, if there is a risk of malignant nodules in the thyroid or
if there are cysts that can be drained.
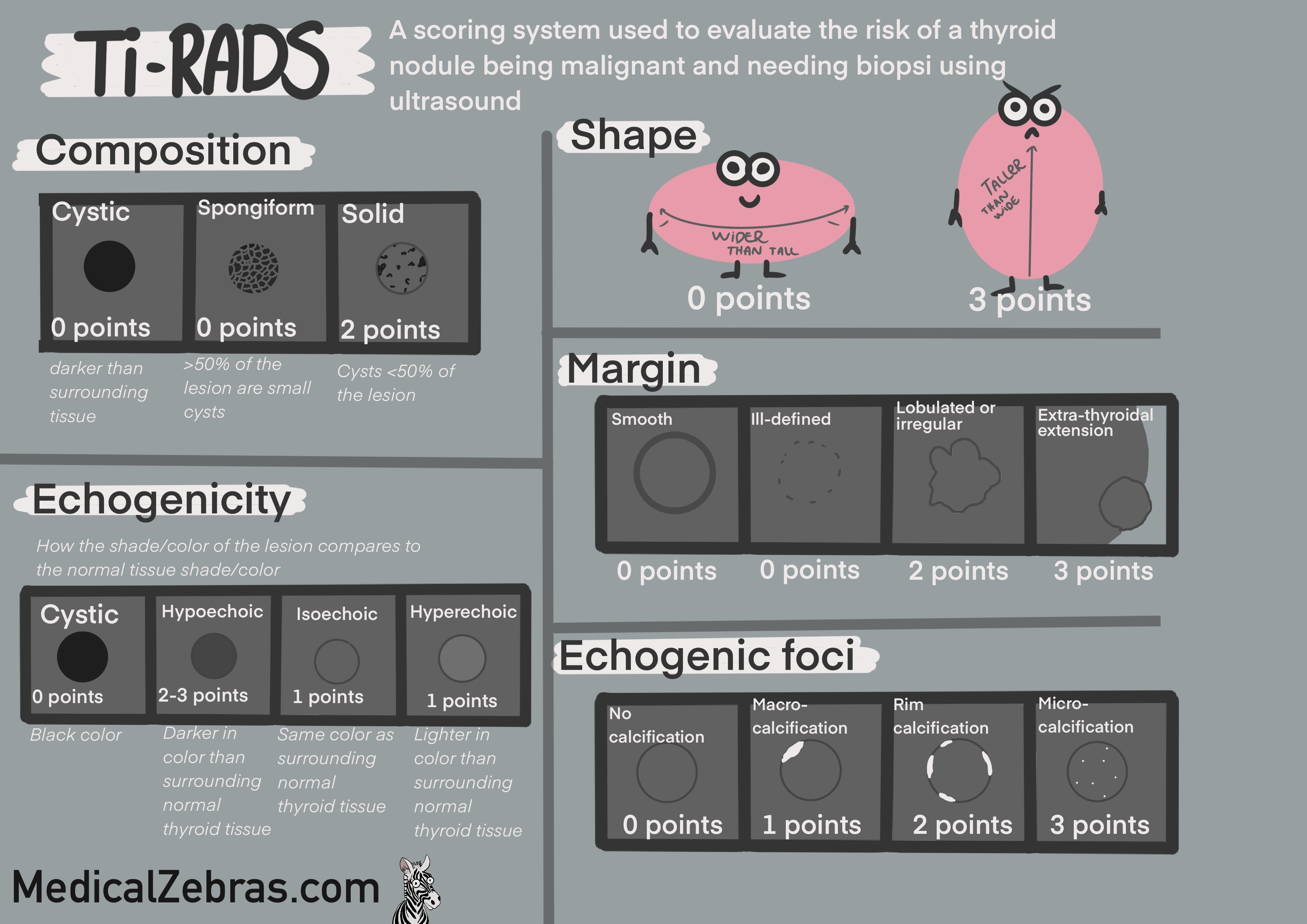
All nodules are classified according to the ACR TI-RADS system (American College of Radiology Thyroid Imaging, Reporting and Data System). This system uses a point system to classify the nodules from TR1-TR5, where TR1 is benign and TR5 is highly suspicious of malignancy. The points are given based on the following criteria:
All nodules are classified according to the ACR TI-RADS system (American College of Radiology Thyroid Imaging, Reporting and Data System). This system uses a point system to classify the nodules from TR1-TR5, where TR1 is benign and TR5 is highly suspicious of malignancy. The points are given based on the following criteria:
-
Composition
-
cystic (0)
-
spongiform (0)
-
mixed cystic and solid (1)
-
solid or almost completely solid(2)
-
Echogenicity
-
anechoic (0)
-
hyperechoic or isoechoic (1)
-
hypoechoic (2)
-
very hypoechoic(3)
-
Shape
-
wider-than-tall (0)
-
taller-than-wide (3)
-
Margin
-
smooth (0)
-
ill-defined(0)
-
lobulated or irregular (2)
-
extra-thyroidal extension (3)
-
Echogenic foci
-
none or large comet-tail artifacts (0)
-
macrocalcifications (1)
-
peripheral (rim) calcifications (2)
-
punctate echogenic foci (3)
Based on the total points, the nodule is classified as follows
& recommendations for FNA:
- TR1 (0 points): Benign => No FNA needed
- TR2 (2 points): Not suspicious => No FNA needed
- TR3 (3 points): Mildly suspicious => FNA if nodule is ≥2.5 cm
- TR4 (4-6 points): Moderately suspicious => FNA if nodule is ≥1.5 cm
- TR5 (7 or more points): Highly suspicious => FNA if nodule is ≥1.0 cm
Pros:
- Great way to easily assess the thyroid tissue structure
- User dependent.
- Might lead to over-diagnosis of small benign nodules, leading to overuse of unnecessary biopsies.
Pathology
Hypothyroidism
Symptoms:
-
Fatigue
-
Weight gain
-
Cold intolerance
-
Constipation
-
Hair thinning
-
Brain fog and depression
-
Bradycardia
-
Dry skin
-
Myxedema (swelling of the skin and underlying tissues)

Hashimoto thyroiditis (Chronic lymphocytic thyroiditis)
an autoimmune condition that causes chronic inflammation of the thyroid gland. It is characterized by gradual destruction of the thyroid tissue, leading to hypothyroidism. The inflammation is caused by the body's immune system attacking the thyroid gland, leading to the production of autoantibodies against thyroid proteins such as thyroglobulin and thyroid peroxidase. This leads to gradual damage to the thyroid tissue, resulting in decreased production of thyroid hormones.- T3 and T4 levels: low
- TSH levels: high
- Anti-thyroid peroxidase (anti-TPO) antibodies: positive
- Anti-thyroglobulin antibodies: positive
- Levothyroxine (synthetic T4) to replace the deficient thyroid hormones.
Diagnosis:
Treatment:
Iodine deficiency hypothyroidism
Iodine deficiency is a common cause of hypothyroidism worldwide, as iodine is an essential component of thyroid hormones. When the body does not get enough iodine from the diet, the thyroid gland cannot produce enough thyroid hormones, leading to hypothyroidism. This is more common in areas where the soil and water are deficient in iodine, such as in mountainous regions or areas far from the sea.- T3 and T4 levels: low
- TSH levels: high
- Urinary iodine concentration: low
- Iodine supplementation through diet or iodine-containing supplements.
- Levothyroxine (synthetic T4) to replace the deficient thyroid hormones.
Diagnosis:
Treatment:
Congenital hypothyroidism
is a condition present at birth where the thyroid gland is either absent, underdeveloped, or not functioning properly. This can lead to a deficiency of thyroid hormones, which are essential for normal growth and development, particularly of the brain. If left untreated, congenital hypothyroidism can lead to intellectual disability and other developmental problems.- T3 and T4 levels: low
- TSH levels: high
- Newborn screening tests: positive
- Levothyroxine (synthetic T4) to replace the deficient thyroid hormones.
Diagnosis:
Treatment:
Postpartum thyroiditis
is an inflammation of the thyroid gland that occurs in some women following childbirth. It is believed to be an autoimmune condition, where the body's immune system attacks the thyroid gland. Postpartum thyroiditis typically occurs within the first year after delivery and can cause temporary hyperthyroidism followed by hypothyroidism.- T3 and T4 levels: initially high, then low
- TSH levels: initially low, then high
- Anti-thyroid peroxidase (anti-TPO) antibodies: positive
- Beta-blockers to manage symptoms of hyperthyroidism (if needed).
- Levothyroxine (synthetic T4) to replace the deficient thyroid hormones (if needed).
Diagnosis:
Treatment:
Drug-induced hypothyroidism
Certain medications can interfere with thyroid hormone production or function, leading to hypothyroidism. Common drugs that can cause hypothyroidism include- lithium (used to treat bipolar disorder),
- amiodarone (used to treat arrhythmias),
- interferon-alpha (used to treat certain viral infections and cancers).
- T3 and T4 levels: low
- TSH levels: high
- Medication history: use of drugs known to cause hypothyroidism
- Discontinuation or adjustment of the offending medication (if possible).
- Levothyroxine (synthetic T4) to replace the deficient thyroid hormones.
Diagnosis:
Treatment:
Iatrogenic hypothyroidism
Iatrogenic hypothyroidism occurs as a result of medical treatment, typically following thyroid surgery (thyroidectomy) or radioactive iodine therapy used to treat hyperthyroidism or thyroid cancer. In these cases, the thyroid gland is either partially or completely removed or destroyed, leading to a deficiency of thyroid hormones.- T3 and T4 levels: low
- TSH levels: high
- Medical history: recent thyroid surgery or radioactive iodine therapy
- Levothyroxine (synthetic T4) to replace the deficient thyroid hormones.
Diagnosis:
Treatment:
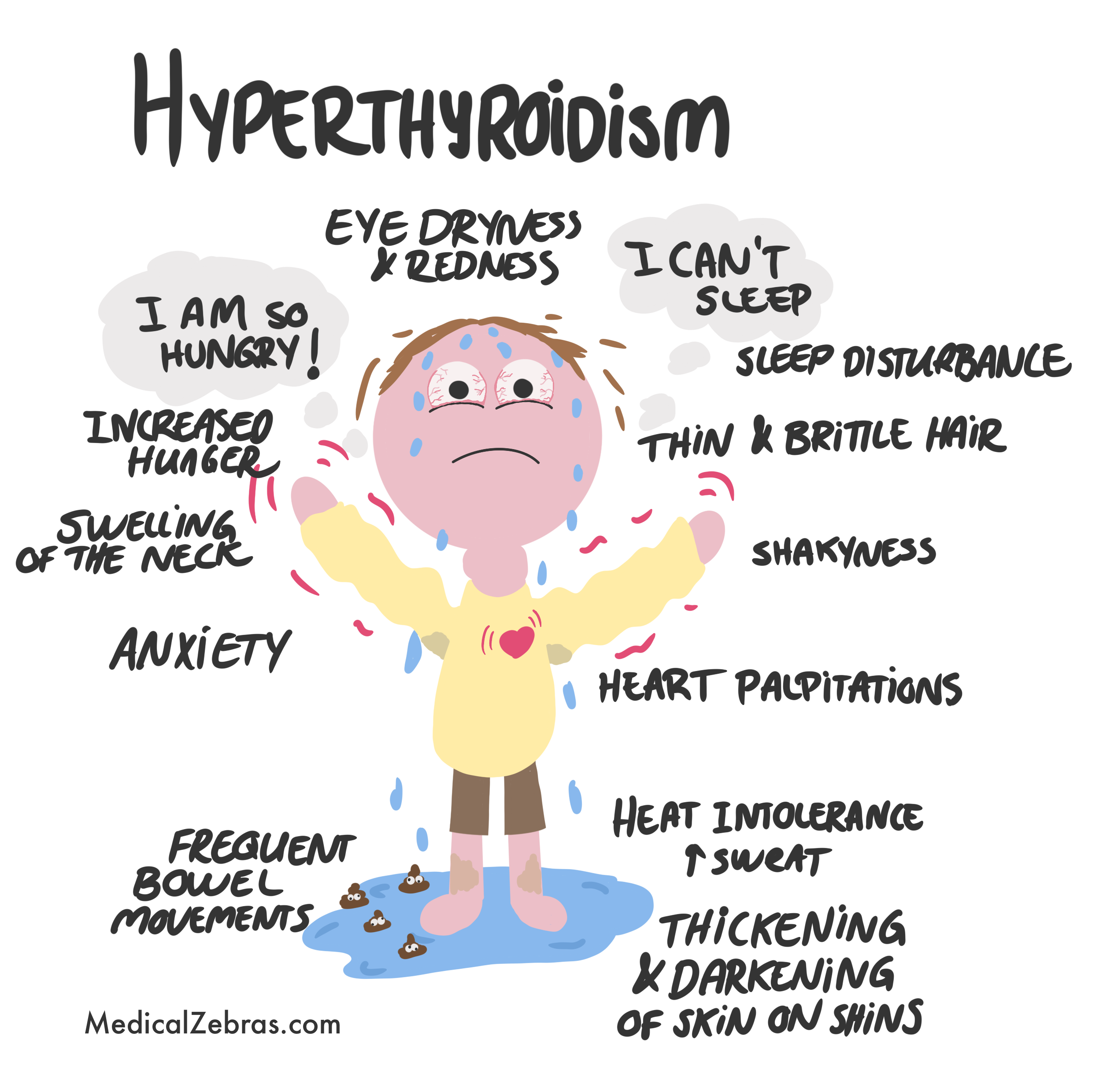
Hyperthyroidism
Symptoms:
-
Anxiety
-
Heart palpitations
-
Heat intolerance
-
Tremors
-
Weight loss
-
Increased appetite
-
Swelling and darkening of shins
-
Thyroid enlargement (goiter)
-
Fatigue
-
Muscle weakness
-
Increased sweating
-
Frequent bowel movements, sometimes diarrhea
-
Menstrual irregularities
-
Exophthalmos (bulging eyes) -
specific to Graves disease, an autoimmune reaction in the
tissues around the eyes. Rare to see now due to early
treatment.
Graves disease
Is when the body produces autoantibodies that stimulate the TSH receptor, causing the thyroid gland to become overactive, and produce too much of the thyroid hormones T3 and T4. This is the most common cause of hyperthyroidism. This is more common in females (3%) than males (0,5%).- T3 and T4 levels: high
- TSH levels: low
- Anti-TSH receptor antibodies (TRAb): positive
- Thyroid scintigraphy: diffuse increased uptake of radioactive iodine throughout the thyroid gland.
- Beta-blockers to manage symptoms such as rapid heart rate and tremors. !important to manage symptoms these symptoms first before starting other treatments!
- Antithyroid medications (such as methimazole or propylthiouracil),
- Radioactive iodine therapy, or surgery (thyroidectomy).
Diagnosis:
Treatment:
Toxic thyroid adenoma
Is when a benign tumor of the thyroid gland produces excess thyroid hormones, leading to hyperthyroidism.- T3 and T4 levels: high
- TSH levels: low
- Anti-TSH receptor antibodies (TRAb): negative
- Thyroid scintigraphy: focal increased uptake of radioactive iodine in the area of the adenoma, with decreased uptake in the rest of the thyroid gland.
- Beta-blockers to manage symptoms such as rapid heart rate and tremors. !important to manage symptoms these symptoms first before starting other treatments!
- Antithyroid medications (such as methimazole or propylthiouracil),
- Radioactive iodine therapy, or surgery (lobectomy).
Diagnosis:
Treatment:
Thyroiditis
Is inflammation of the thyroid gland, which can be caused by a variety of factors, including infections, autoimmune diseases, and certain medications (for example amiodarone). There are several types of thyroiditis, including:- Subacute thyroiditis (de Quervain thyroiditis): is a self-limiting condition that often follows a viral infection. It is characterized by a painful, tender thyroid gland, and symptoms of hyperthyroidism followed by hypothyroidism. The inflammation causes the release of pre-formed thyroid hormones into the bloodstream, leading to symptoms of hyperthyroidism. As the inflammation resolves, the thyroid gland may become temporarily underactive, leading to symptoms of hypothyroidism. Most patients recover fully within a few months.
- Silent thyroiditis (painless thyroiditis): is an autoimmune condition that causes inflammation of the thyroid gland without pain. It is characterized by symptoms of hyperthyroidism followed by hypothyroidism, similar to subacute thyroiditis. However, there is no tenderness or pain in the thyroid gland. Most patients recover fully within a few months.
Malignant pathology
Follicular carcinoma
- Prevalence: ~10% of all diagnosed thyroid cancers, but prevalence varies greatly according to study and population (from 5% to even 30%). Generally good prognosis, but worse than papillary thyroid carcinoma. More aggressive and more likely to metastasize via the bloodstream (to lungs and bones) than papillary thyroid carcinoma.
- Risk: radiation exposure, iodine deficiency.
-
Histology: follicules made up of cuboidal cells (like
normal thyroid follicles), but the lesion is surrounded by a
fibrous capsule that is often thickened and sometimes irregular.
The follicles can be small or large and the cells can be arranged
in a microfollicular, trabecular, or solid pattern. The cells can
have varying degrees of atypia, with enlarged nuclei and prominent
nucleoli. The diagnosis of follicular carcinoma is based on the
presence of capsular and/or vascular invasion, which can be
difficult to assess on fine-needle aspiration biopsy. Therefore, a
surgical excision is needed to make the diagnosis.
- positive for thyroglobulin and TTF-1, and many other markers.
-
Genetics: most often you will find somatic mutations in the RAS
gene and/or the PAX8-PPARγ1 translocation. Both of these mutations
lead to activation of the MAPK and PI3K/AKT signaling pathways,
which promote cell growth and division.
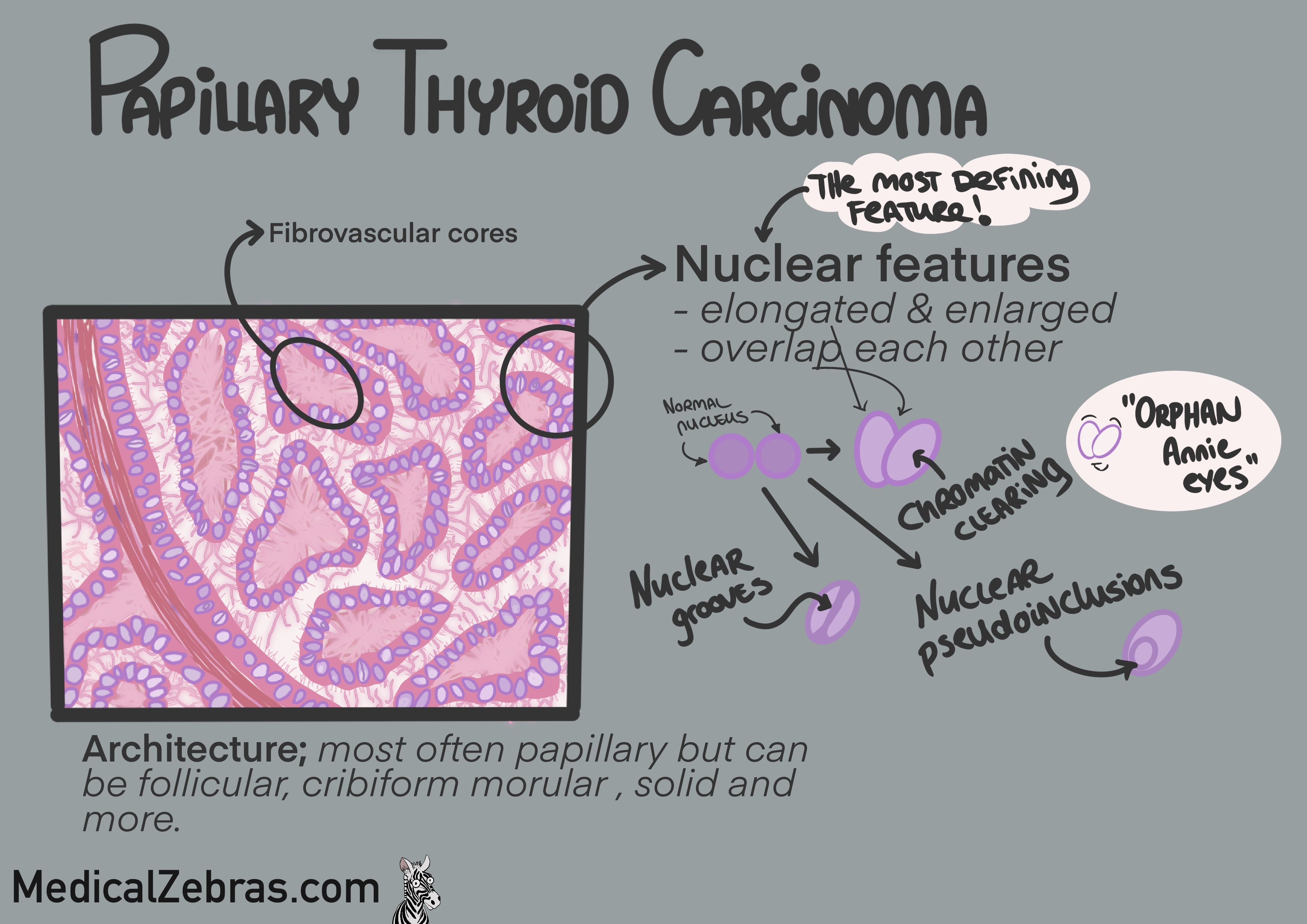
Papillary thyroid carcinoma
- Prevalence: 80-90% af all diagnosed thyroid cancers. Excellent prognosis. Aggressiveness seems to be uncertain, as autopsy studies have shown about 10% of people have small papillary thyroid carcinomas that never caused any symptoms or problems during their lifetime.
- Risk: increased risk in those who have been exposed to radiation or have a history of thyroid disease (such as goiter).
-
Histology: is mostly based on nuclear morphology; the
nuclei overlap each other and are enlarged and elongated/oval with
central clearing (often referred to as Annie´s eyes). The nuclei
can have grooves and inclusions. The cells are often arranged in
papillary structures, hence the name, with fibrovascular cores.
You can also sometimes see psammoma bodies (concentric
calcifications).
- positive for thyroglobulin and TTF-1.
-
Genetics: most often caused by mutations in the BRAF gene
(especially BRAF V600E) or RET/PTC rearrangements.
Both of these mutations lead to activation of the MAPK signaling
pathway, which promotes cell growth and division. BRAF V600E seems
to be associated with a more aggressive form of papillary thyroid
carcinoma, with a higher risk of recurrence and metastasis.
Medullary carcinoma
- Prevalence: about 5% of all thyroid cancers diagnosed, but rapports range from 1-10%. 25% of the cases are hereditary (MEN2A, MEN2B or familial medullary thyroid carcinoma (FMTC)). The prognosis is worse than for papillary and follicular thyroid carcinoma, but better than for anaplastic thyroid carcinoma.
- Risk: generally radiation exposure and those with congenital mutation in the RET-gene (MEN2A, MEN2B or FMTC).
-
Histology: the cancer originates from the parafollicular
cells or the "C-cells" and is therefore a neuroendocrine tumor as
the C-cells are of neural crest origin. The cells are often
arranged in solid nests, trabeculae, sheets or even follicles, and
the cells can have a variety of shapes, including spindle-shaped,
polygonal, or plasmacytoid. The cytoplasm can be granular ("salt
and pepper") or clear, and the nuclei can be round or oval with
prominent nucleoli. Amyloid deposits are often present in the
stroma, which can be detected with Congo red staining. Sometimes
you will find mucin.
- positive for calcitonin, CEA, chromogranin A and synaptophysin.
-
Genetics: certain mutations in the RET gene cause
hereditary syndrome MEN2A, MEN2B and Familial MTC, which is
associated with a high risk of developing medullary thyroid
carcinoma. These mutations lead to activation of the RET tyrosine
kinase receptor, which promotes cell growth and division. Sporadic
cases of medullary thyroid carcinoma can also have mutations in
the RET gene, as well as in other genes such as RAS and BRAF.
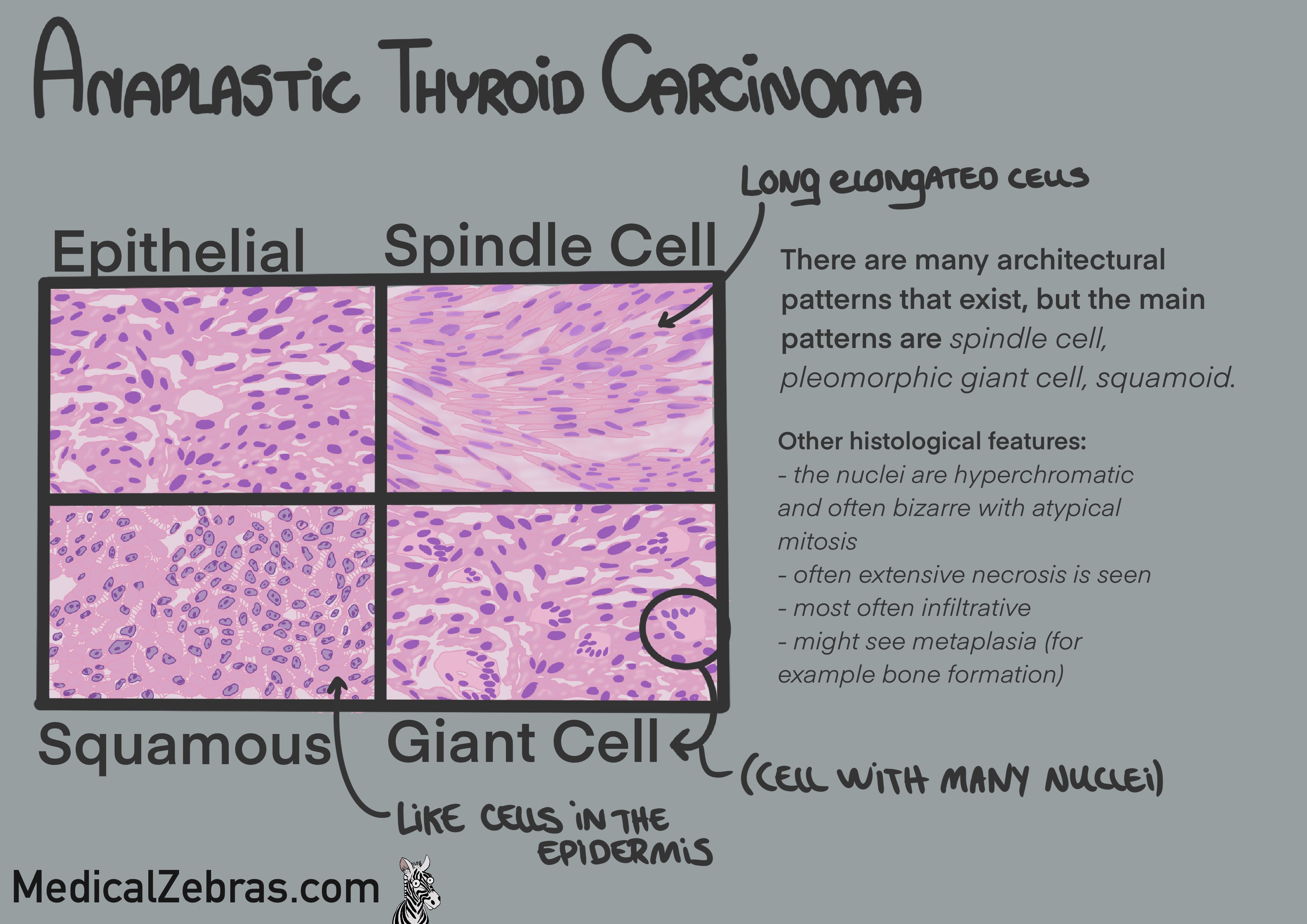
Anaplastic carcinoma
- Prevalence: 1-2% of all thyroid cancers and rare. Highly aggressive and locally invasive.
- Risk: as it is so rare, the risk factors are not well understood.
-
Histology: the cells are undifferentiated and can have many
different shapes and sizes, including spindle-shaped, giant, or
squamoid. The cells can be arranged in sheets, nests, or
trabeculae, and the cytoplasm can be abundant or scant. The nuclei
are often pleomorphic and hyperchromatic, with prominent nucleoli.
Mitoses are often numerous, and necrosis is common. The tumor can
invade surrounding tissues, including blood vessels and nerves.
- often positive for p53, Ki-67 (high proliferation index), and cytokeratins, but negative for thyroglobulin and TTF-1.
-
Genetics: associated with many somatic mutations, for
example in TERT (telomere gene), TP53 (oncogene), BRAF, RAS, and
PIK3CA. These mutations lead to activation of various signaling
pathways, including MAPK and PI3K/AKT, which promote cell growth
and division. Considered somatic (and not hereditary) in most
cases.