Anatomy, histology and physiology
The parathyroid glands are four small glands located on the back
of the thyroid gland in the neck. They are typically about the
size of a grain of rice (approximately 6 mm in length and 3-4 mm
in width) and are usually found in pairs, with two glands on
each thyroid lobe. However, the number and location of
parathyroid glands can vary among individuals, and some people
may have more or fewer than four glands. As they are small, they
cannot be seen on imaging studies such as ultrasound or CT
scans, or during autopsy, unless they are enlarged due to
disease.
There are some imaging techniques, such as sestamibi scans, where a radioactive materiale attached to sestamibi (Tc99-sestamibi) is used to visualise the glands as it is taken up by oxyphil cells in the parathyroid gland and correlates with the activity and number of mitochondria in the cell, meaning that the more hyperactive the cell is, the more potent the uptake is. However if the hyperactivity is mainly because of growth of chief cells, the glands are harder to visualise with this technique. This imaging technique it is not routinely used to visualise normal parathyroid glands, only if pathology is suspected.
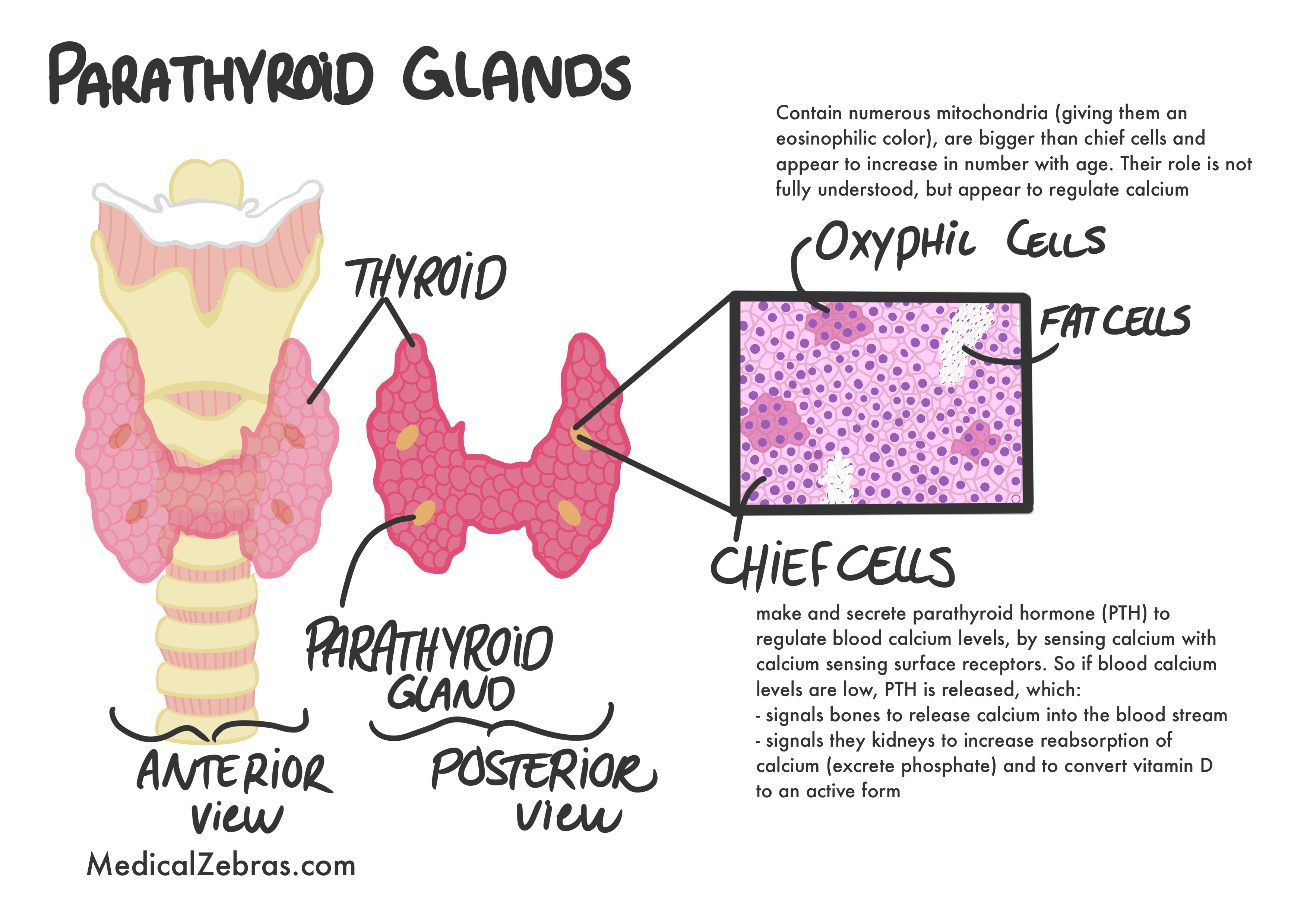
The parathyroid glands are responsible for regulating calcium levels in the blood and bone metabolism. They achieve this by producing and secreting parathyroid hormone (PTH), which increases blood calcium levels by stimulating the release of calcium from bones, increasing calcium absorption in the intestines, and reducing calcium excretion by the kidneys.
There are some imaging techniques, such as sestamibi scans, where a radioactive materiale attached to sestamibi (Tc99-sestamibi) is used to visualise the glands as it is taken up by oxyphil cells in the parathyroid gland and correlates with the activity and number of mitochondria in the cell, meaning that the more hyperactive the cell is, the more potent the uptake is. However if the hyperactivity is mainly because of growth of chief cells, the glands are harder to visualise with this technique. This imaging technique it is not routinely used to visualise normal parathyroid glands, only if pathology is suspected.
The parathyroid glands are responsible for regulating calcium levels in the blood and bone metabolism. They achieve this by producing and secreting parathyroid hormone (PTH), which increases blood calcium levels by stimulating the release of calcium from bones, increasing calcium absorption in the intestines, and reducing calcium excretion by the kidneys.
Histology:
The parathyroid gland is composed of tightly packed cells with little intervening stroma. The chief cells are small, polygonal cells with a centrally located nucleus and a pale cytoplasm. The oxyphil cells are larger and have a more eosinophilic cytoplasm due to their high mitochondrial content. The gland is highly vascularized, with numerous capillaries and sinusoids running between the cells. In between the clusters of chief and oxyphil cells, there are also adipocytes (fat cells) present, which increase in number with age. The parathyroid glands are composed of two main types of cells:- Chief cells: These cells are the most abundant and are responsible for producing and secreting PTH. Chief cells contain numerous secretory granules that store PTH until it is needed.
- Oxyphil cells: These cells are larger and less numerous than chief cells. They contain high levels of mitochondria which gives them their characteristic eosinophilic (pink) appearance on histological sections. Their exact function is not fully understood, but they are thought to play a role in the metabolism of PTH or in the regulation of calcium levels.
Embryology:
-
Third pharyngeal pouch => Inferior parathyroid
glands.
-
Migrate with the thymus and descend lower in the neck,
ending up below the superior parathyroid glands. Because
of this, the inferior parathyroid glands have a more
variable location than the superior parathyroid glands.
Can sometimes be found in the thymus or even the
mediastinum (ectopic locations).
-
Fourth pharyngeal pouch =>
Superior parathyroid glands.
-
Migrate with the thyroid gland and end up at the level
of the upper poles of the thyroid gland.
The parathyroid glands are derived from the endodermal lining
of the third and fourth pharyngeal pouches. The glands appear
around 5th week of gestation and are fully developed by the
6th week.
Genetics
Multiple Endocrine Neoplasia type 1 (MEN1):
Autosomal dominant
MEN1 gene, which codes for the protein menin, a tumor suppressor.
Symptoms: tumors in multiple endocrine glands
MEN1 gene, which codes for the protein menin, a tumor suppressor.
- Parathyroid tumors are typically multiple and adenomatous.
- Pituitary gland tumors are often functional, meaning they produce hormones (for example prolactin or growth hormone)
- Pancreas tumors are most often neuroendocrine tumors and can be both benign and malignant. Gastrinomas and insulinomas are the most common ones associated.
Multiple Endocrine Neoplasia type 2A (MEN2A):
Autosomal dominant
RET gene which affects cell growth and differentiation.
Symptoms:
RET gene which affects cell growth and differentiation.
- Parathyroid hyperplasia that causes hypercalcemia (increased PTH)
- Medullary thyroid carcinoma that produces calcitonin (C cells)
- Pheochromocytoma is a tumor in the adrenal gland that produces too much epinephrine and norepinephrine
Familial Isolated Hyperparathyroidism:
Autosomal dominant
CDC73 gene. Leads to overproduction of PTH.
Symptoms:
CDC73 gene. Leads to overproduction of PTH.
- Hypercalcemia (bone pain, kidney stones, nausea, fatigue)
Familial hypocalciuric hypercalcemia (FHH)
Autosomal dominant
CaSR gene that codes for a calcium sensing receptor that is found on chief cells of the parathyroid and cells lining the kidney tubule. Important for regulating PTH secretion and renal calcium excretion.
Symptoms: PTH is inappropriately normal/high despite
elevated calcium.
CaSR gene that codes for a calcium sensing receptor that is found on chief cells of the parathyroid and cells lining the kidney tubule. Important for regulating PTH secretion and renal calcium excretion.
- Mild hypercalcemia due to altered set point for calcium sensing => decreased PTH suppression
- Hypocalciuria (low calcium in urine) due to increased renal reabsorption of calcium
- Usually asymptomatic
DiGeorge syndrome (22q11.2 deletion):
22q11.2 deletion
The third and fourth pharyngeal pouches are affected
- Parathyroid hypoplasia or aplasia => hypocalcemia, even convulsions if severe
- Thymic hypoplasia => defective T cell system and recurrent infections
- Cardiac defects such as Tetralogy of Fallot, truncus arteriosus, and interrupted aortic arch
- Cleft palate
- Learning difficulties
- Mild facial features, such as a small mouth, hooded eyelids, low-set ears, and a prominent nose
Autosomal dominant hypophosphatemic rickets
FGF23 gene
-
Symptoms:
- Hypophosphatemia due to renal phosphate wasting (decreased tubular phosphate reabsorption)
- Normal PTH and calcium levels
- Osteomalacia, rickets, small stature, lower limb deformities.
Pathology
Hyperparathyroidism
This condition is characterized by excessive PTH secretion, leading to elevated blood calcium levels (hypercalcemia). It can be caused by a benign tumor (adenoma) in one of the parathyroid glands (primary hyperparathyroidism), or as a compensatory response to low blood calcium levels due to chronic kidney disease or vitamin D deficiency (secondary hyperparathyroidism).
Symptoms:
A common memonic to remember the symptoms of hypercalcemia is
-
Hypercalcemia symptoms:
may present with symptoms such as
- Kidney stones: often made of calcium oxalate or calcium phosphate and can cause severe pain in the back or side, blood in the urine, and frequent urination.
- Bone pain: due to increased bone resorption caused by elevated PTH levels. This can lead to osteoporosis and an increased risk of fractures.
- Fatigue: often due to muscle weakness and lethargy caused by hypercalcemia.
- Gastrointestinal disturbances (nausea, constipation): caused by hypercalcemia affecting the smooth muscle function of the gastrointestinal tract.
- Neuropsychiatric symptoms (depression, confusion, delirium, even psychosis) as it causes reduced neuronal excitability.
- Osteopenia/osteoporosis: thinning of the bones, especially in the spine, hips and wrists, which increases fracture risk.
"stones, bones, groans, and psychiatric overtones,"
which refers to kidney stones, bone pain, abdominal discomfort, and
neuropsychiatric symptoms such as confusion and depression.
Types of hyperparathyroidism:
-
Primary hyperparathyroidism: This is the most common form
of hyperparathyroidism and is usually caused by a benign tumor
(adenoma) in one of the parathyroid glands. It can also be caused
by hyperplasia (enlargement) of all four glands or, rarely, by
parathyroid carcinoma. Often only one gland is affected, leading
to excessive PTH secretion and hypercalcemia. 85% of cases are due
to a single parathyroid adenoma, 10-15% are due to parathyroid
hyperplasia, and less than 1% are due to parathyroid carcinoma.
90% of primary hyperparathyroidism cases are sporadic, while 10%
are familial, associated with genetic syndromes such as Multiple
Endocrine Neoplasia type 1 (MEN1), Multiple Endocrine Neoplasia
type 2A (MEN2A), and Familial Isolated Hyperparathyroidism.
-
Diagnosis:
-
Blood test:
-
Serum Calcium:
high
-
PTH:
normal/high
-
Phosphate:
low/normal
-
ALP:
elevated (increased bone turnover)
-
Ultrasound or sestamibi scans to locate the affected
parathyroid gland(s).
-
Treatment:
- Asymptomatic patients with mild hypercalcemia: monitoring of serum calcium and bone density, along with lifestyle modifications such as adequate hydration, weight-bearing exercise, and avoiding medications that can increase calcium levels (e.g., thiazide diuretics).
-
Symptomatic patients or those with significant
hypercalcemia:
-
First step is
hydration with intravenous fluids
to help lower blood calcium levels.
-
Bisphosphonates/denosumab
to inhibit bone resorption and lower blood calcium levels,
by preventing osteoclast activity that is stimulated by
PTH. osteoclasts are the cells responsible for breaking
down bone tissue and releasing calcium into the
bloodstream.
-
Calcimimetics
like Cinacalcet to lower PTH production, by increasing the
sensitivity of calcium-sensing receptors on the
parathyroid glands to extracellular calcium levels. This
leads to decreased PTH secretion and subsequently lowers
blood calcium levels.
-
Surgery:
removal of the affected parathyroid gland(s) is the
definitive treatment for primary hyperparathyroidism.
-
Minimally invasive parathyroidectomy
is the preferred surgical approach, which involves
removing only the affected gland(s) through a small
incision in the neck. Intraoperative PTH monitoring can
be used to confirm successful removal of the affected
gland(s).
-
Secondary hyperparathyroidism: This occurs as a
compensatory response to chronic hypocalcemia, often due to
chronic kidney disease or vitamin D deficiency. In this condition,
all four parathyroid glands are usually enlarged and secrete
excess PTH in an attempt to raise blood calcium levels. In the
case of chronic kidney disease, the kidneys are unable to convert
vitamin D to its active form (calcitriol), leading to decreased
calcium absorption from the intestines and hypocalcemia.
Additionally, the kidneys are unable to excrete phosphate, leading
to hyperphosphatemia, which further stimulates PTH secretion.
-
Kidney failure causes phosphate retention and reduced vitamin D
activation → low calcium → increased PTH.
-
Diagnosis:
-
Blood tests:
-
Serum Calcium:
low/normal
-
PTH:
high
-
Phosphate:
high (in chronic kidney disease)
-
ALP:
may be elevated (increased bone turnover)
-
Vitamin D:
low
-
Kidney function tests:
to assess for chronic kidney disease
-
Treatment:
-
Medical management:
-
First step is
correcting hypocalcemia
with calcium and vitamin D supplementation.
-
Phosphate binders
to reduce phosphate levels in the blood (in chronic kidney
disease).
-
Calcimimetics
like Cinacalcet to lower PTH levels.
-
Surgical intervention:
may be necessary if medical management is ineffective or if
there are complications such as severe bone disease
(osteopenia, osteoporosis and in severe cases osteitis
fibrosa cystica where bone is replaced by fibrous tissue and
cyst-like brown tumors).
-
Blood tests:
-
Tertiary hyperparathyroidism: This occurs when secondary
hyperparathyroidism becomes autonomous and continues to secrete
excess PTH even after the underlying cause of hypocalcemia has
been corrected. This is most commonly seen in patients with
long-standing chronic kidney disease who have undergone kidney
transplantation.
-
Diagnosis:
-
Blood tests:
-
Serum Calcium:
high
-
PTH:
high
-
Phosphate:
can be low/normal
-
ALP:
elevated (increased bone turnover)
-
Vitamin D:
low
- Imaging studies: ultrasound or sestamibi scans to assess the size and function of the parathyroid glands.
-
Treatment:
-
Medical management:
-
First step is
correcting any residual hypocalcemia
with calcium and vitamin D supplementation.
-
Calcimimetics
like Cinacalcet to lower PTH levels.
-
Phosphate binders
to reduce phosphate levels in the blood.
- Surgical intervention: may be necessary if medical management is ineffective or if there are complications such as severe hypercalcemia or bone disease (osteopenia, osteoporosis and in severe cases osteitis fibrosa cystica where bone is replaced by fibrous tissue and cyst-like brown tumors).
-
Blood tests:
Hungry bone syndrome
is a condition that can occur after removal of the parathyroid glands after a prolonged hypercalcemia because of high PTH. After the surgery, suddenly the PTH level drops that leads to increased osteoblast (cells that form bone) activity increased calcium bone absorption that in turn decreases calcium levels in the blood (as the bones are "hungry" after a proloned destruction and are now "eating" up blood calcium when PTH is no longer affecting them).
Symptoms:
- Bone pain
- Symptoms of hypocalcemia (see above)
Diagnosis:
- same as hypocalcemia. The hypocalcemia tends to be profound (very low serum calcium)
Treatment:
- same as hypocalcemia (see above)
Osteitis fibrosa cystica
is a severe form of bone disease that can occur in the setting of hyperparathyroidism, particularly in cases of primary or tertiary hyperparathyroidism. It is characterized by increased bone resorption due to excessive PTH secretion, leading to weakened bones that are prone to fractures and deformities.In osteitis fibrosa cystica, the excessive PTH stimulates osteoclasts, the cells responsible for bone resorption, leading to increased breakdown of bone tissue. This results in the release of calcium and phosphate into the bloodstream, contributing to hypercalcemia. The increased bone resorption also leads to the formation of cyst-like lesions in the bones, which are filled with fibrous tissue and can be seen on X-rays as "brown tumors" due to the presence of hemosiderin (a breakdown product of blood). These lesions can weaken the bones and make them more susceptible to fractures.
Symptoms:
- Bone pain and tenderness
- Fractures, especially in the long bones and vertebrae
- Skeletal deformities, such as bowed legs or spinal curvature (kyphosis)
- Muscle weakness
- Fatigue
Diagnosis:
-
Blood tests:
-
Serum Calcium:
high
-
PTH:
high
-
Phosphate:
low/normal
-
ALP:
elevated (increased bone turnover)
- Imaging studies: X-rays may show subperiosteal bone resorption (especially in the phalanges), cyst-like brown tumors, and generalized osteopenia (reduced bone density).
- Bone biopsy: may be performed to confirm the diagnosis and assess the extent of bone involvement.
Treatment:
- Addressing the underlying cause of hyperparathyroidism: This may involve surgical removal of the affected parathyroid gland(s) in cases of primary hyperparathyroidism or medical management in cases of secondary or tertiary hyperparathyroidism.
- Medical management: This may include bisphosphonates to inhibit bone resorption, calcium and vitamin D supplementation to support bone health, and pain management for bone pain.
- Monitoring and follow-up: Regular monitoring of serum calcium and PTH levels, as well as bone density assessments, is important to assess treatment response and prevent further bone complications.
Maternal hyperparathyroidism
is a condition that occurs when a pregnant woman has hyperparathyroidism, leading to elevated levels of calcium in her blood. This can have significant implications for both the mother and the developing fetus. Maternal hyperparathyroidism can be caused by primary hyperparathyroidism (due to a parathyroid adenoma or hyperplasia) or secondary hyperparathyroidism (due to chronic kidney disease or vitamin D deficiency). During pregnancy, the maternal body undergoes various physiological changes that can affect calcium metabolism, including increased calcium absorption from the intestines and increased calcium transfer to the fetus. This can exacerbate the effects of hyperparathyroidism, leading to more pronounced hypercalcemia. The elevated calcium levels in the mother can cross the placenta and affect the fetus, potentially leading to fetal hypercalcemia and suppression of the fetal parathyroid glands. This can result in neonatal hypocalcemia after birth, as the newborn's parathyroid glands may be temporarily suppressed and unable to produce sufficient PTH to maintain normal calcium levels.Symptoms: are similar to those of hypercalcemia in non-pregnant individuals (see above).
Hypoparathyroidism
This condition is characterized by insufficient PTH secretion, leading to low blood calcium levels (hypocalcemia). It can be caused by surgical removal of the parathyroid glands (e.g., during thyroid surgery), autoimmune destruction of the glands, or genetic disorders ( e.g., DiGeorge syndrome (22q11.2 deletion - affects the gland development), or mutations in the GCM2 gene which is important for parathyroid development leading to congenital hypoparathyroidism - called familial isolated hypoparathyroidism).
Symptoms:
-
-
Acute hypoparathyroidism:
may present with severe hypocalcemia and symptoms such as:
- Chvostek's sign (twitching of facial muscles when the facial nerve is tapped),
- Trousseau's sign (carpal spasm induced by inflating a blood pressure cuff above systolic pressure for several minutes).
- Carpopedal spasms (involuntary contractions of the hands and feet),
- Laryngospasm (spasmodic closure of the vocal cords leading to breathing difficulties),
- cognitive disturbances such as confusion and irritability,
- seizures (due to increased neuronal excitability),
- cardiac arrhythmias (due to prolonged QT interval on ECG).
-
Tetany
(muscle cramps and spasms),
-
Paresthesias
(tingling sensations in the hands, feet, and around the
mouth),
- Chronic hypoparathyroidism: may present with milder symptoms such as muscle cramps, fatigue, and anxiety.
A common mnemonic to remember the symptoms of hypocalcemia is
"CATS go numb," which refers to
- C - Convulsions (seizures)
- A - Arrhythmias (irregular heartbeats)
- T - Tetany (muscle cramps and spasms)
- S - Spasms and numbness (tingling sensations)
Diagnosis:
-
Blood tests:
-
Serum Calcium:
low
-
Serum PTH:
low or inappropriately normal
-
Serum Phosphorus:
high
-
Also measure: Magnesium as hypomagnesemia can cause functional
hypoparathyroidism, as well as kidney function tests to rule
out other causes of hypocalcemia, as low albumin levels can
also lead to low total calcium levels.
Treatment:
- Acute management: iv calcium gluconate for severe hypocalcemia. This is usually administered slowly to avoid cardiac complications and it is important to monitor serum calcium levels closely during iv calcium administration.
-
Chronic management:
- Oral calcium supplements (e.g., calcium carbonate or calcium citrate, such as Tums and Caltrate as well as dietary calcium intake ( dairy products, leafy green vegetables, fortified foods)).
- Active vitamin D analogs (e.g., calcitriol) to enhance calcium absorption. These are preferred over regular vitamin D (cholecalciferol or ergocalciferol) as they do not require activation by the kidneys (PTH is needed for the last step of activation of vitamin D in the kidneys).
- Monitoring of serum calcium and phosphorus levels to avoid hypercalcemia and hyperphosphatemia.
Hypomagnesemia
Low magnesium levels can lead to functional hypoparathyroidism by impairing PTH secretion and action. Magnesium is essential for the proper functioning of the parathyroid glands, and low magnesium levels can lead to decreased PTH secretion and impaired calcium regulation.
Symptoms:
- Symptoms of hypocalcemia (see above)
- Muscle cramps
- Fatigue
- Weakness
Diagnosis:
-
Blood tests:
-
Serum Magnesium:
low
-
Serum Calcium:
low
-
Serum PTH:
low or inappropriately normal
Treatment:
- Magnesium supplementation: oral or intravenous magnesium to correct hypomagnesemia.
- Calcium supplementation: may be necessary to correct hypocalcemia until magnesium levels are normalized.
Parathyroid carcinoma
This is an extremely rare malignant tumor (< 0.005% of all cancers worldwide) of the parathyroid glands that can cause severe hypercalcemia due to excessive PTH secretion. It may present with a palpable neck mass, hoarseness, and difficulty swallowing, as it presses on adjacent structures in the neck. There are very few cases of parathyroid carcinoma reported in the literature, and it accounts for less than 1% of all cases of hyperparathyroidism. 90% of parathyroid carcinomas are functional tumors that secrete excess PTH, leading to severe hypercalcemia. The remaining 10% are non-functional tumors that do not produce PTH. 50% of patients with parathyroid carcinoma present with a palpable neck mass, which is uncommon in benign parathyroid adenomas. 25-30% of patients with parathyroid carcinoma may present with hoarseness or difficulty swallowing due to invasion of the recurrent laryngeal nerve or esophagus. 10% of patients with parathyroid carcinoma may have a family history of hyperparathyroidism-jaw tumor syndrome, a rare genetic disorder that predisposes to parathyroid carcinoma. 5-year survival rate for parathyroid carcinoma is approximately 85%, but the 10-year survival rate drops to around 50% due to recurrence and metastasis. 30-40% of patients with parathyroid carcinoma will experience local recurrence after initial surgery, and 10-15% will develop distant metastases, most commonly to the lungs and bones.Genetics: The majority of parathyroid carcinomas are sporadic, but a small percentage (less than 1%) are associated with genetic syndromes such as hyperparathyroidism-jaw tumor syndrome (caused by a mutation in CDC73 (or HRPT2)) and multiple endocrine neoplasia type 1 (gene MEN1).
Histology: There is no specific histological feature that definitively distinguishes parathyroid carcinoma from benign parathyroid adenomas. However, certain features such as capsular invasion, vascular invasion, and mitotic activity may suggest malignancy.
Symptoms:
- Severe hypercalcemia symptoms ( stones, bones, groans, and psychiatric overtones )
- Palpable neck mass
- Hoarseness
- Difficulty swallowing
- Bone pain
- Kidney stones
- Fatigue
- Gastrointestinal disturbances
Diagnosis:
-
Blood tests:
-
Serum Calcium:
very high
-
PTH:
markedly elevated (often >3-10 times the upper limit of
normal)
- Imaging studies: ultrasound, sestamibi scan, CT or MRI to locate the tumor and assess for local invasion or metastasis
- Biopsy: may be performed to confirm the diagnosis, although it is not always necessary if clinical and imaging findings are suggestive of parathyroid carcinoma.
Treatment:
- Surgery: en bloc resection of the tumor and affected parathyroid gland(s) with clear margins is the primary treatment for parathyroid carcinoma.
- Adjuvant therapy: may be considered in cases of incomplete resection or metastatic disease, although its effectiveness is limited.