Anatomy, histology and physiology
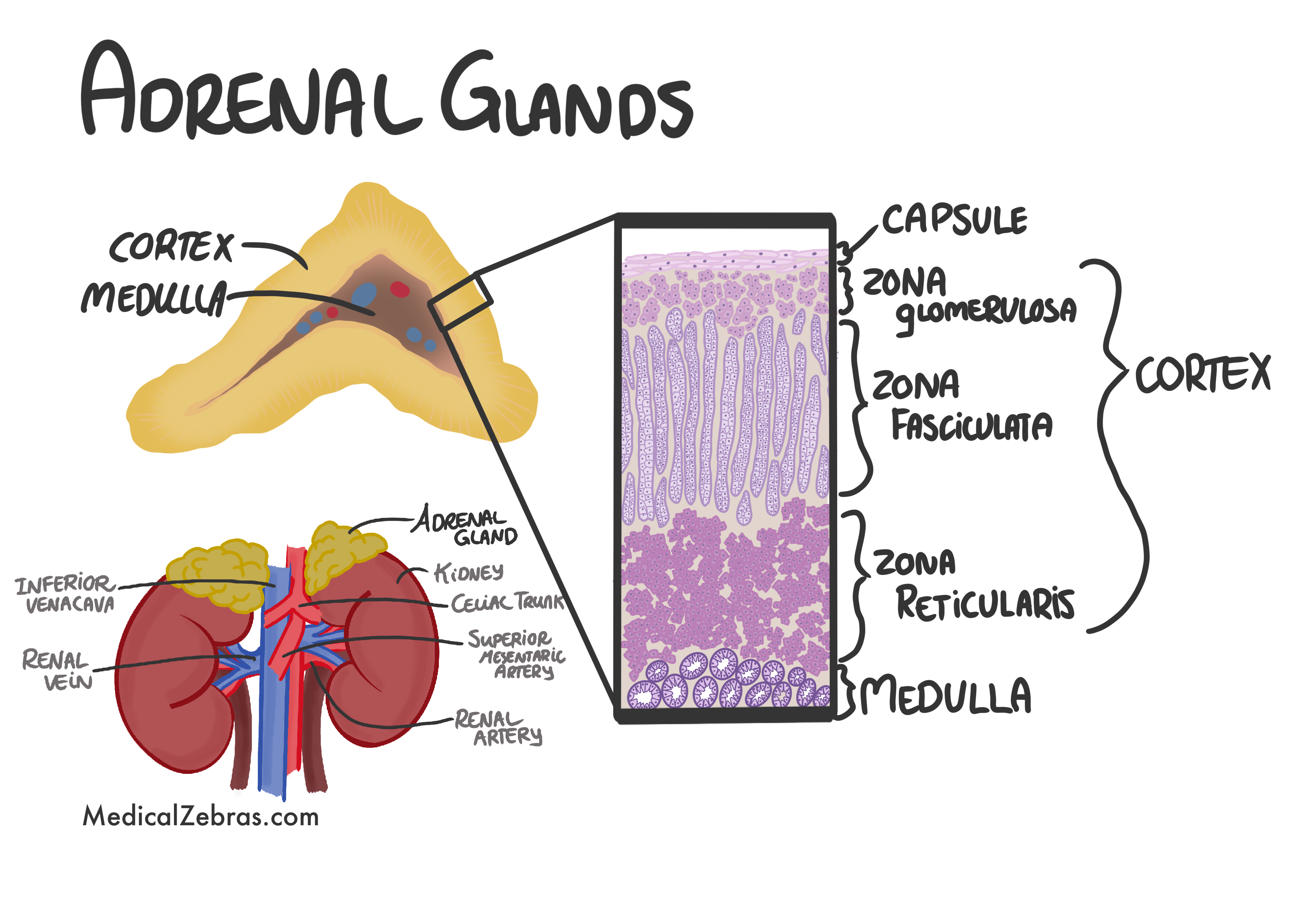
The adrenal glands are small yellowish, triangular-shaped glands
located on top of each kidney. They are part of the endocrine
system and play a crucial role in producing hormones that
regulate various bodily functions, including metabolism, immune
response, blood pressure, and stress response.
Each adrenal gland consists of two main parts: the outer cortex and the inner medulla.
The cortex is divided into three layers:
Each adrenal gland consists of two main parts: the outer cortex and the inner medulla.
The cortex is divided into three layers:
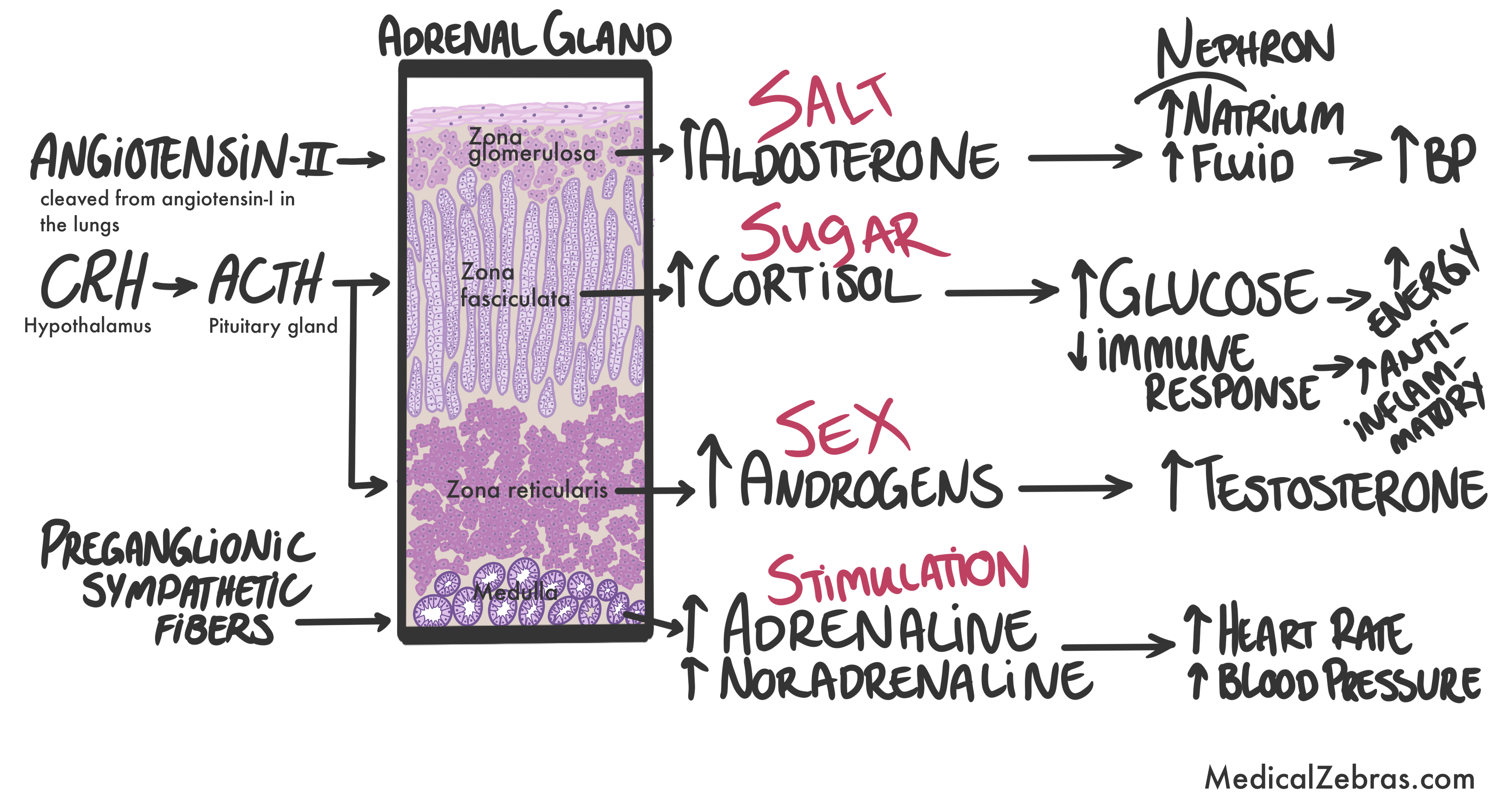
- Zona glomerulosa: The outermost layer, responsible for producing mineralocorticoids, such as aldosterone. Aldosterone acts on the kidneys, more specifically on the distal tubules and collecting ducts, where it promotes sodium retention (and with that water reabsorption) and potassium excretion. This leads to an increase in blood volume and thus a higher blood pressure.
- Zona fasciculata: The middle layer, produces glucocorticoids, such as cortisol. Cortisol is secreted in response to stress and low blood-glucose levels, and it has several important functions, including increasing blood sugar through gluconeogenesis (in the liver), suppressing the immune system (anti-inflammatory effects), and aids in fat, protein, and carbohydrate metabolism. Too much cortisol can lead to Cushing's syndrome, while too little can cause Addison's disease.
- Zona reticularis: The innermost layer, responsible for producing androgens, mainly dehydroepiandrosterone (DHEA) and androstenedione. These hormones are than converted into more potent androgens, such as testosterone, and estrogens in the gonads and other tissues. Androgens play a role in the development of secondary sexual characteristics and influence libido.
- Adrenaline (epinephrine): This hormone is released in response to stress and helps prepare the body for a "fight or flight" response by increasing heart rate, blood pressure, and blood flow to muscles. It also helps increase blood sugar levels by promoting glycogenolysis in the liver.
- Noradrenaline (norepinephrine): This hormone works alongside adrenaline to increase heart rate and blood pressure, and it also helps regulate blood vessel constriction.
Pathology
Addison's disease (adrenal insufficiency)
is a rare disorder that occurs when the adrenal glands do not produce enough of the hormones cortisol and aldosterone. This can be caused by autoimmune diseases, infections, or other factors that damage the adrenal glands, such as tuberculosis, metastatic cancer or hemorrhage due to trauma, infection or surgery.
Symptoms:
- Fatigue and weakness
- Weight loss and decreased appetite
- Low blood pressure, which may cause dizziness or fainting
- Hyperpigmentation (darkening of the skin)
- Salt cravings
- Nausea, vomiting, and diarrhea
- Muscle and joint pain
Diagnosis:
- Blood tests to measure cortisol and ACTH levels
- ACTH stimulation test to assess adrenal function
- Imaging studies (CT scan, MRI) to evaluate adrenal gland size and structure
Treatment:
- Hormone replacement therapy with corticosteroids (e.g., hydrocortisone) and mineralocorticoids (e.g., fludrocortisone)
- Management of underlying causes (e.g., infections, autoimmune diseases)
- Stress management and education on adrenal crisis prevention
Cushing's syndrome
is a condition that occurs when there is an excess of cortisol in the body. This can be caused by long-term use of corticosteroid medications or by tumors in the pituitary gland or adrenal glands that produce too much cortisol.
Symptoms:
- Weight gain, particularly around the abdomen and face
- Thin skin that bruises easily
- Muscle weakness
- High blood pressure
- Osteoporosis (weakening of the bones)
- Mood changes, such as irritability or depression
- Increased thirst and urination
Causes:
- Prolonged use of corticosteroid medications (exogenous Cushing's syndrome)
- Pituitary adenomas producing excess ACTH (Cushing's disease)
- Adrenal tumors producing excess cortisol
- Ectopic ACTH production by non-pituitary tumors (e.g., small cell lung cancer)
Diagnosis:
- 24-hour urinary free cortisol test
- Low-dose dexamethasone suppression test
- Blood tests to measure cortisol and ACTH levels
- Imaging studies (CT scan, MRI) to locate tumors in the pituitary or adrenal glands
Treatment:
- Surgical removal of tumors (pituitary or adrenalectomy)
- Medications to control cortisol production (e.g., ketoconazole, metyrapone)
- Gradual tapering of corticosteroid medications if they are the cause
- Management of symptoms and complications (e.g., hypertension, osteoporosis)
Pheochromocytoma
is a rare tumor that develops in the adrenal medulla and produces excess catecholamines (adrenaline and noradrenaline). This can lead to high blood pressure and other symptoms.
Histology:
- Pheochromocytomas arise from the chromaffin cells of the adrenal medulla, which are derived from neural crest cells.
- Grossly, pheochromocytomas are typically well-circumscribed, encapsulated masses that can vary in size from a few millimeters to several centimeters. They may appear brownish or reddish due to the presence of catecholamines and their metabolites.
- Microscopically, pheochromocytomas are characterized by nests of polygonal cells with abundant granular cytoplasm, arranged in a "zellballen" pattern (small nests or clusters) separated by a rich vascular network. The cells have round to oval nuclei with prominent nucleoli. Mitotic figures may be present, and areas of necrosis or hemorrhage can also be observed in some cases.
Genetics:
Pheochromocytomas can be sporadic or associated with hereditary
syndromes such as
- Multiple Endocrine Neoplasia type 2 (MEN2) => RET gene mutations
- Von Hippel-Lindau disease => VHL gene mutations
- Neurofibromatosis type 1 (NF1) => NF1 gene mutations
Symptoms:
- High blood pressure (hypertension)
- Headaches
- Sweating
- Rapid heartbeat (tachycardia)
- Tremors
- Paleness (pallor)
- Shortness of breath Symptoms tend to occur in sudden, severe episodes (paroxysms) lasting from minutes to hours.
Diagnosis:
- Blood tests:
- Adrenaline and noradrenaline levels: elevated.
- 24-hour urine collection to measure catecholamine levels
- Imaging studies (CT scan, MRI, MIBG scan) to locate the tumor
Treatment:
- Surgical removal of the tumor (adrenalectomy)
- Preoperative management with alpha-blockers and beta-blockers to control blood pressure and heart rate
- Regular follow-up to monitor for recurrence or metastasis